

Severe asthma: definition, diagnosis and treatment
- PMID: 25585581
- PMCID: PMC4357024
- DOI: 10.3238/arztebl.2014.0847
Severe asthma: definition, diagnosis and treatment
Abstract
Background: A minority of patients with asthma have uncontrolled or partially controlled asthma despite intensive treatment. These patients present a special challenge because of the extensive diagnostic evaluation that they need, insufficient evidence regarding personalized treatments, and their high consumption of health-care resources.
Methods: The definition, diagnosis, and treatment of severe asthma are presented on the basis of a selective literature review and the authors' clinical experience.
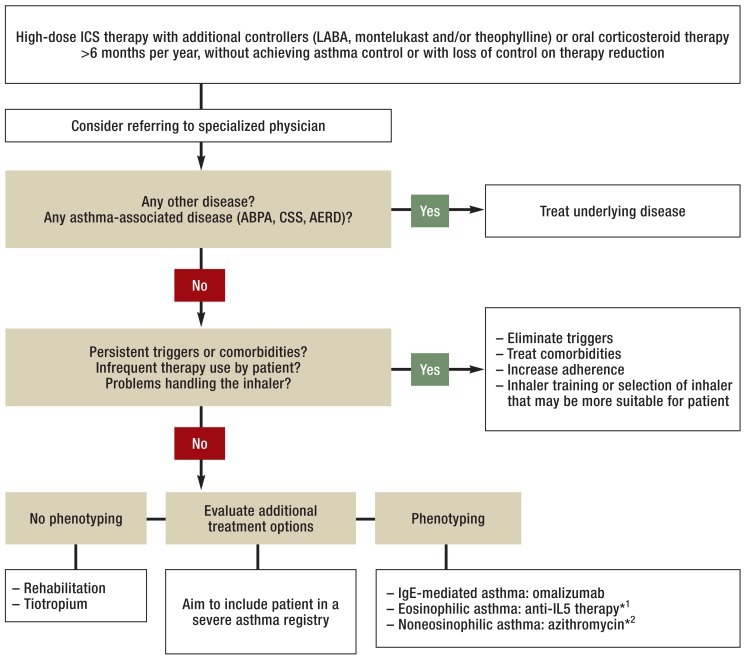
Results: Severe asthma is present, by definition, when adequate control of asthma cannot be achieved by high-dose treatment with inhaled cortico - steroids and additional controllers (long-acting inhaled beta 2 agonists, montelukast, and/or theophylline) or by oral corticosteroid treatment (for at least six months per year), or is lost when the treatment is reduced. Before any further treatments are evaluated, differential diagnoses of asthma should be ruled out, comorbidities should be treated, persistent triggers should be eliminated, and patient adherence should be optimized. Moreover, pulmonary rehabilitation is recommended in order to stabilize asthma over the long term and reduce absences from school or work. The additional drugs that can be used include tiotropium, omalizumab (for IgE-mediated asthma), and azithromycin (for non-eosinophilic asthma). Antibodies against interleukin-5 or its receptor will probably be approved soon for the treatment of severe eosinophilic asthma.
Conclusion: The diagnosis and treatment of severe asthma is time consuming and requires special experience. There is a need for competent treatment centers, continuing medical education, and research on the prevalence of severe asthma.
Figures
Comment in
-
Marginal Effect and Little Clinical Relevance.Dtsch Arztebl Int. 2015 Aug 31;112(35-36):601. doi: 10.3238/arztebl.2015.0601a. Dtsch Arztebl Int. 2015. PMID: 26377532 Free PMC article. No abstract available.
-
Polysomnographic Screening Helpful.Dtsch Arztebl Int. 2015 Aug 31;112(35-36):601. doi: 10.3238/arztebl.2015.0601b. Dtsch Arztebl Int. 2015. PMID: 26377533 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2015 Aug 31;112(35-36):601-2. doi: 10.3238/arztebl.2015.0601c. Dtsch Arztebl Int. 2015. PMID: 26377534 Free PMC article. No abstract available.
References
-
- Sears MR. Trends in the prevalence of asthma. Chest. 2014;145:219–225. - PubMed
-
- Rackemann FM. A clinical study of one hundred and fifty cases of bronchial asthma. Arch Intern Med. 1918;12:517–552.
-
- Jia CE, Zhang HP, Lv Y, et al. The asthma control test and asthma control questionnaire for assessing asthma control: Systematic review and meta-analysis. J Allergy Clin Immunol. 2013;131:695–703. - PubMed
-
- Rowe BH, Voaklander DC, Wang D, et al. Asthma presentations by adults to emergency departments in Alberta, Canada: A large population-based study. Chest. 2009;135:57–65. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical