

First-in-man phase 1 clinical trial of gene therapy for advanced pancreatic cancer: safety, biodistribution, and preliminary clinical findings
- PMID: 25586689
- PMCID: PMC4395782
- DOI: 10.1038/mt.2015.1
First-in-man phase 1 clinical trial of gene therapy for advanced pancreatic cancer: safety, biodistribution, and preliminary clinical findings
Abstract
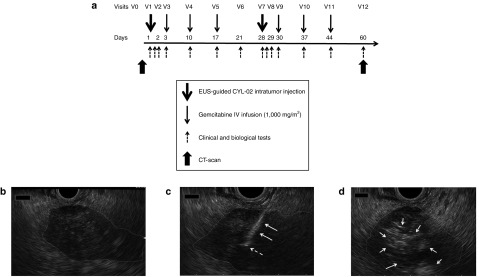
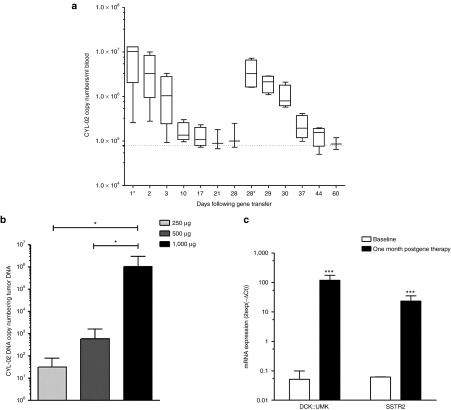
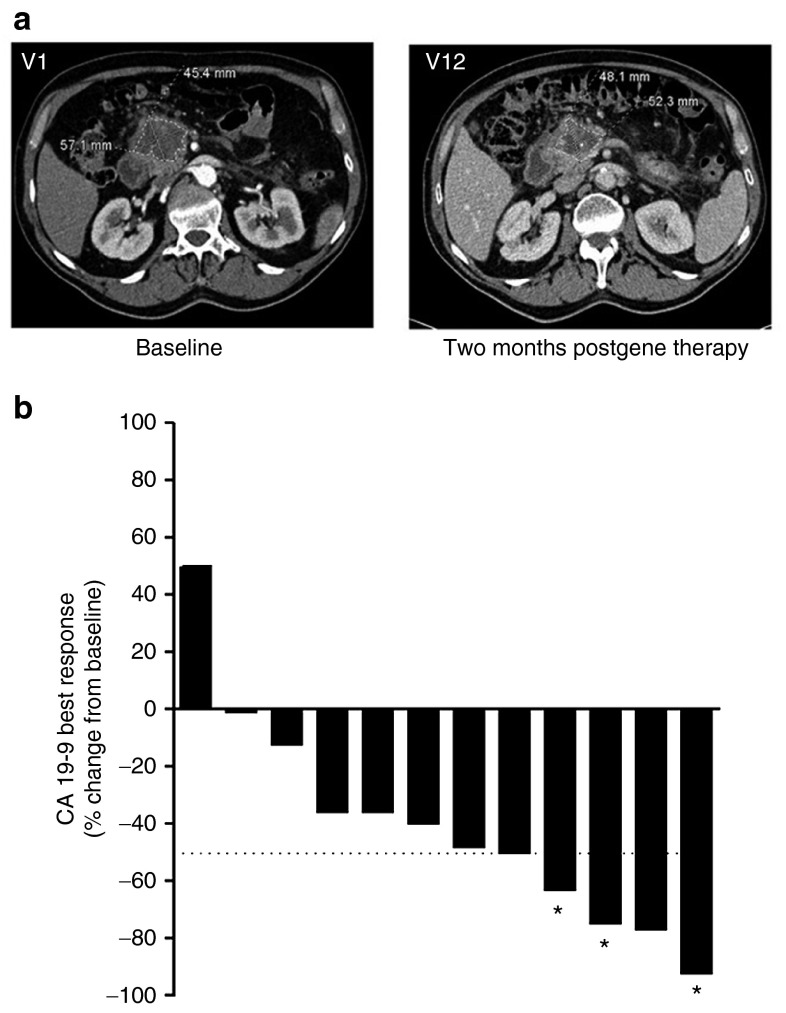
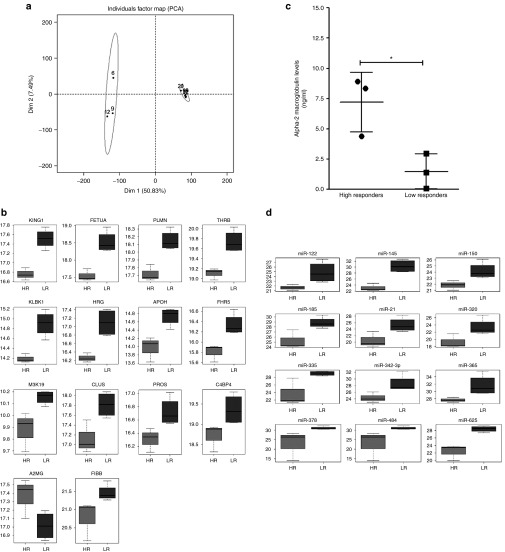
This phase 1 trial was aimed to determine the safety, pharmacokinetics, and preliminary clinical activity of CYL-02, a nonviral gene therapy product that sensitizes pancreatic cancer cells to chemotherapy. CYL-02 was administrated using endoscopic ultrasound in 22 patients with pancreatic cancer that concomitantly received chemotherapy (gemcitabine). The maximum-tolerated dose (MTD) exceeded the maximal feasible dose of CYL-02 and was not identified. Treatment-related toxicities were mild, without serious adverse events. Pharmacokinetic analysis revealed a dose-dependent increase in CYL-02 DNA exposure in blood and tumors, while therapeutic RNAs were detected in tumors. No objective response was observed, but nine patients showed stable disease up to 6 months following treatment and two of these patients experienced long-term survival. Panels of plasmatic microRNAs and proteins were identified as predictive of gene therapy efficacy. We demonstrate that CYL-02 nonviral gene therapy has a favorable safety profile and is well tolerated in patients. We characterize CYL-02 biodistribution and demonstrate therapeutic gene expression in tumors. Treated patients experienced stability of disease and predictive biomarkers of response to treatment were identified. These promising results warrant further evaluation in phase 2 clinical trial.
Figures
References
-
- Cancer Facts & Figures 2013 . < http://www.cancer.org/research/cancerfactsfigures/cancerfactsfigures/can... >.
-
- Burris HA, 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15:2403–2413. - PubMed
-
- Pancreatic Cancer Action Network . < http://www.pancan.org/ >.
-
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. National Cancer Institute of Canada Clinical Trials Group Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–1966. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
