

Voluntary peer review as innovative tool for quality improvement in the intensive care unit--a retrospective descriptive cohort study in German intensive care units
- PMID: 25587245
- PMCID: PMC4270273
- DOI: 10.3205/000202
Voluntary peer review as innovative tool for quality improvement in the intensive care unit--a retrospective descriptive cohort study in German intensive care units
Abstract
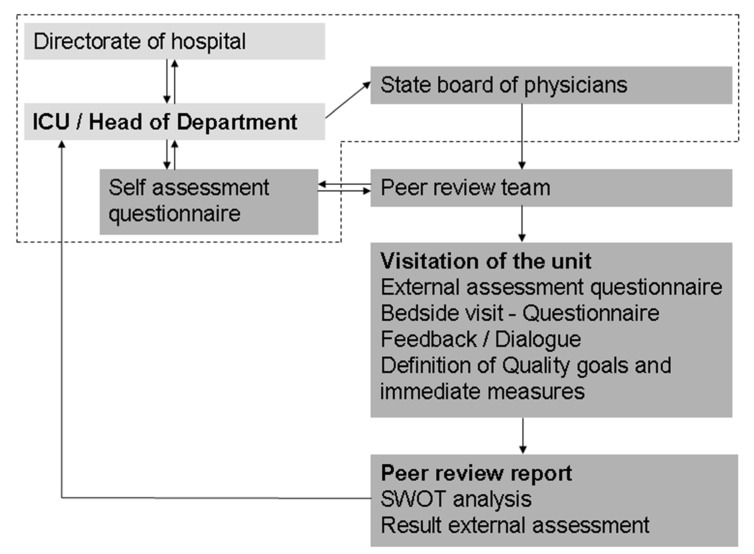
Introduction: Quality improvement and safety in intensive care are rapidly evolving topics. However, there is no gold standard for assessing quality improvement in intensive care medicine yet. In 2007 a pilot project in German intensive care units (ICUs) started using voluntary peer reviews as an innovative tool for quality assessment and improvement. We describe the method of voluntary peer review and assessed its feasibility by evaluating anonymized peer review reports and analysed the thematic clusters highlighted in these reports.
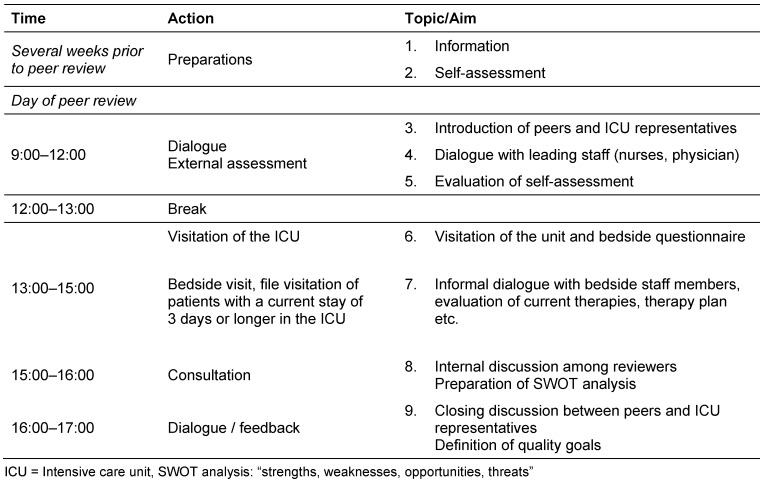
Methods: Retrospective data analysis from 22 anonymous reports of peer reviews. All ICUs - representing over 300 patient beds - had undergone voluntary peer review. Data were retrieved from reports of peers of the review teams and representatives of visited ICUs. Data were analysed with regard to number of topics addressed and results of assessment questionnaires. Reports of strengths, weaknesses, opportunities and threats (SWOT reports) of these ICUs are presented.
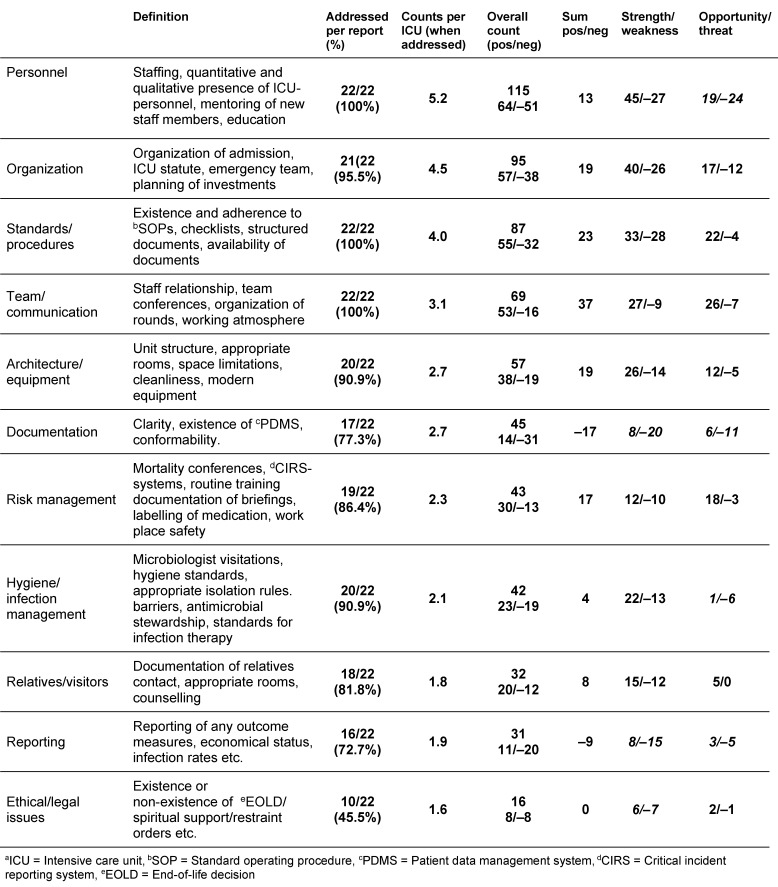
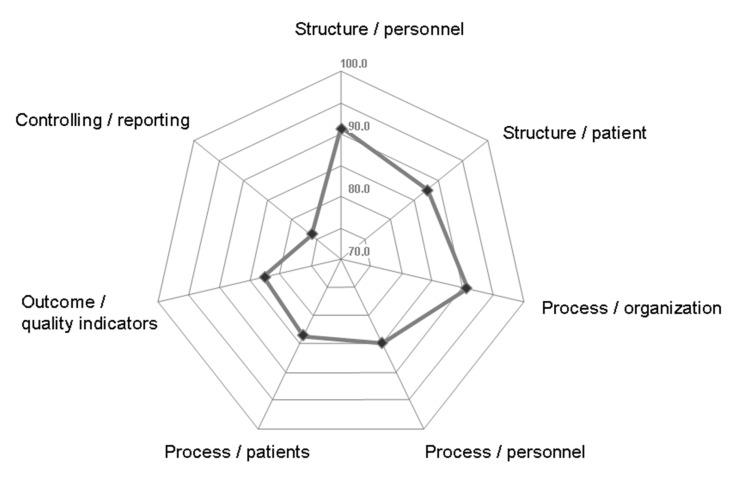
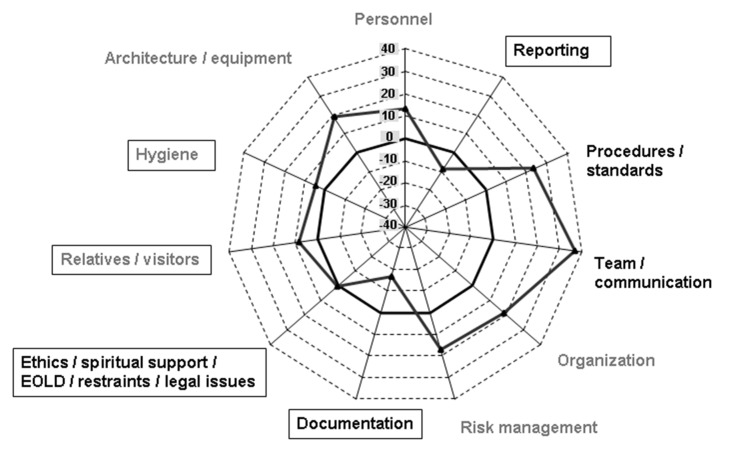
Results: External assessment of structure, process and outcome indicators revealed high percentages of adherence to predefined quality goals. In the SWOT reports 11 main thematic clusters were identified representative for common ICUs. 58.1% of mentioned topics covered personnel issues, team and communication issues as well as organisation and treatment standards. The most mentioned weaknesses were observed in the issues documentation/reporting, hygiene and ethics. We identified several unique patterns regarding quality in the ICU of which long-term personnel problems und lack of good reporting methods were most interesting Conclusion: Voluntary peer review could be established as a feasible and valuable tool for quality improvement. Peer reports addressed common areas of interest in intensive care medicine in more detail compared to other methods like measurement of quality indicators.
Einleitung: Die Verbesserung von Qualität und Sicherheit in der Intensivmedizin gewinnt zunehmend an Bedeutung. Allerdings fehlt ein Goldstandard für die Beurteilung von Qualitätsverbesserung in der Intensivmedizin. Im Jahr 2007 begann ein Pilotprojekt auf deutschen Intensivstationen, das freiwilliges Peer Review als innovatives Instrument zur Qualitätsbewertung und -verbesserung nutzt. Wir beschreiben die Methode des freiwilligen Peer Review und untersuchten ihre Durchführbarkeit. Wir analysierten anonymisierte Peer-Review-Berichte auf die thematischen Schwerpunkte, die in den Berichten hervorgehoben waren. Methode: Retrospektive Datenanalyse von 22 anonymisierten Peer-Review-Berichten. Alle 22 Intensivstationen – mit zusammen mehr als 300 Patientenbetten – hatten sich freiwilligen Peer Reviews unterzogen. Die Daten wurden aus den Berichten der Peer Reviewer und aus den Rückmeldungen der besuchten Intensivstationen gewonnen. Die Daten wurden im Hinblick auf die Anzahl der behandelten Themen und die Ergebnisse der Bewertungsbögen analysiert. Berichte über Stärken, Schwächen, Chancen und Risiken (SWOT-Berichte) dieser Intensivstationen werden vorgestellt. Ergebnisse: Die Bewertung der Struktur, Prozess- und Ergebnisindikatoren zeigte einen hohen Erreichungsgrad der vorgegebenen Qualitätsziele. In den SWOT-Berichten wurden 11 Hauptthemen, die auf allen besuchten Intensivstationen als relevant eingestuft wurden, identifiziert. 58,1% der genannten Themen betrafen Personalfragen, Team- und Kommunikationsfragen sowie Organisation und Behandlungsstandards. Als Schwachstellen wurden die Themen Dokumentation/Reporting, Hygiene und Ethik eingestuft. Fazit: Das freiwillige intensivmedizinische Peer Review stellte sich als einfach anwendbares und wertvolles Instrument für die Qualitätsverbesserung heraus. Die Peer-Review-Berichte behandelten allgemeine Problemschwerpunkte in der Intensivmedizin detaillierter als andere Methoden, wie z.B. die ausschließliche Messung von Qualitätsindikatoren.
Keywords: critical care; patient safety; peer review; quality improvement; quality management.
Figures

References
-
- Dodek PM, Wong H, Jaswal D, Heyland DK, Cook DJ, Rocker GM, Kutsogiannis DJ, Dale C, Fowler R, Ayas NT. Organizational and safety culture in Canadian intensive care units: relationship to size of intensive care unit and physician management model. J Crit Care. 2012 Feb;27(1):11–17. doi: 10.1016/j.jcrc.2011.07.078. Available from: http://dx.doi.org/10.1016/j.jcrc.2011.07.078. - DOI - DOI - PubMed
-
- Valentin A, Capuzzo M, Guidet B, Moreno RP, Dolanski L, Bauer P, Metnitz PG Research Group on Quality Improvement of European Society of Intensive Care Medicine; Sentinel Events Evaluation Study Investigators. Patient safety in intensive care: results from the multinational Sentinel Events Evaluation (SEE) study. Intensive Care Med. 2006 Oct;32(10):1591–1598. doi: 10.1007/s00134-006-0290-7. Available from: http://dx.doi.org/10.1007/s00134-006-0290-7. - DOI - DOI - PubMed
-
- Berenholtz SM, Dorman T, Ngo K, Pronovost PJ. Qualitative review of intensive care unit quality indicators. J Crit Care. 2002 Mar;17(1):1–12. doi: 10.1053/jcrc.2002.33035. Available from: http://dx.doi.org/10.1053/jcrc.2002.33035. - DOI - DOI - PubMed
-
- Najjar-Pellet J, Jonquet O, Jambou P, Fabry J. Quality assessment in intensive care units: proposal for a scoring system in terms of structure and process. Intensive Care Med. 2008 Feb;34(2):278–285. doi: 10.1007/s00134-007-0883-9. Available from: http://dx.doi.org/10.1007/s00134-007-0883-9. - DOI - DOI - PubMed
-
- Braun JP, Bause H, Bloos F, Geldner G, Kastrup M, Kuhlen R, Markewitz A, Martin J, Mende H, Quintel M, Steinmeier-Bauer K, Waydhas C, Spies C NeQuI (quality network in intensive care medicine) Peer reviewing critical care: a pragmatic approach to quality management. GMS Ger Med Sci. 2010;8:Doc23. doi: 10.3205/000112. Available from: http://dx.doi.org/10.3205/000112. - DOI - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
