

Pathologies of the larynx and trachea in childhood
- PMID: 25587369
- PMCID: PMC4273170
- DOI: 10.3205/cto000112
Pathologies of the larynx and trachea in childhood
Abstract
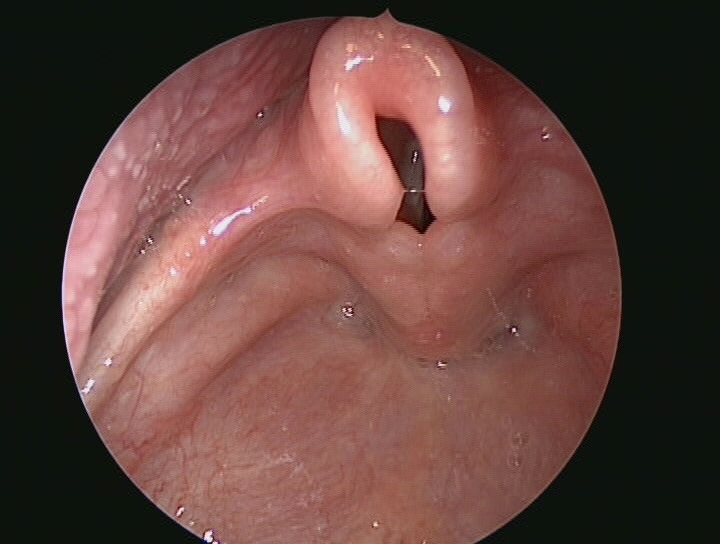
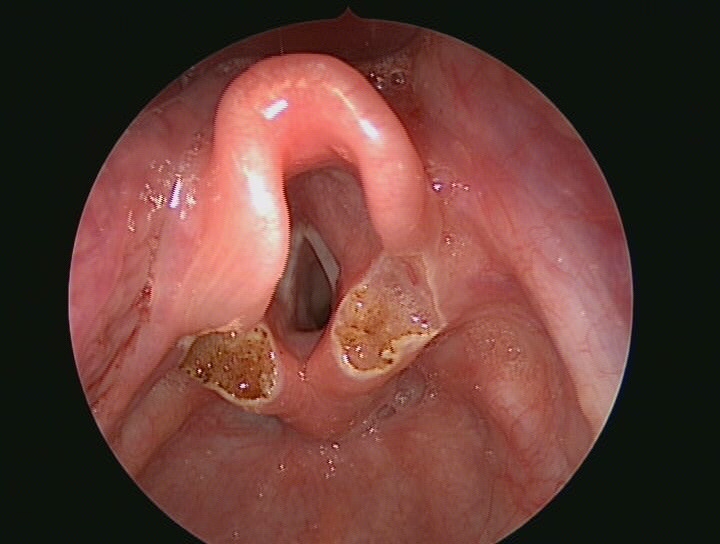
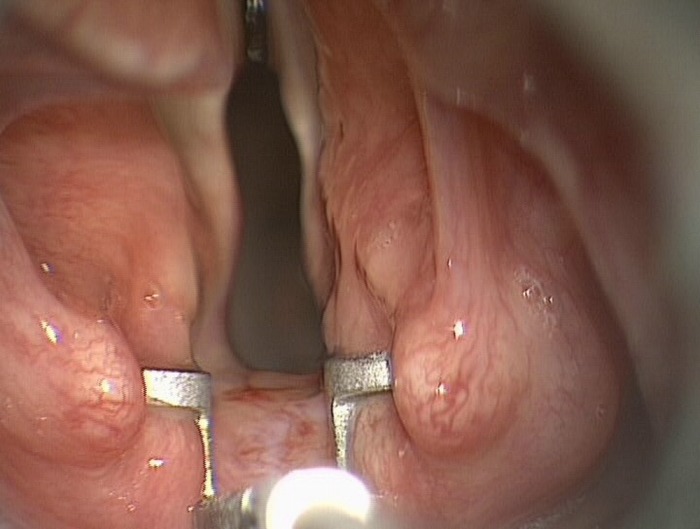
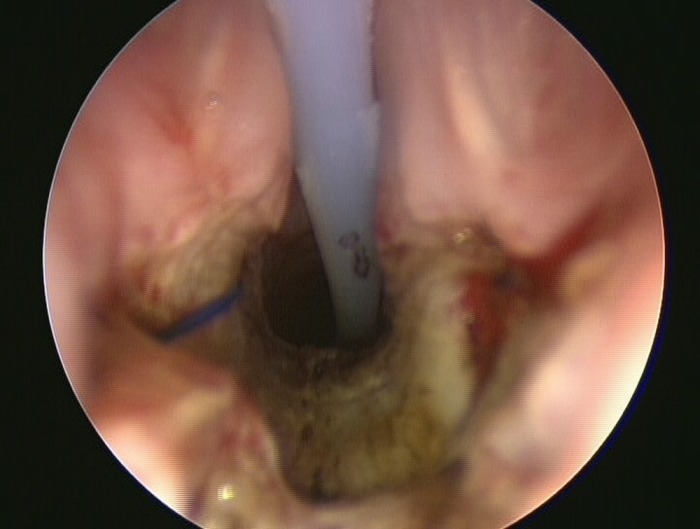
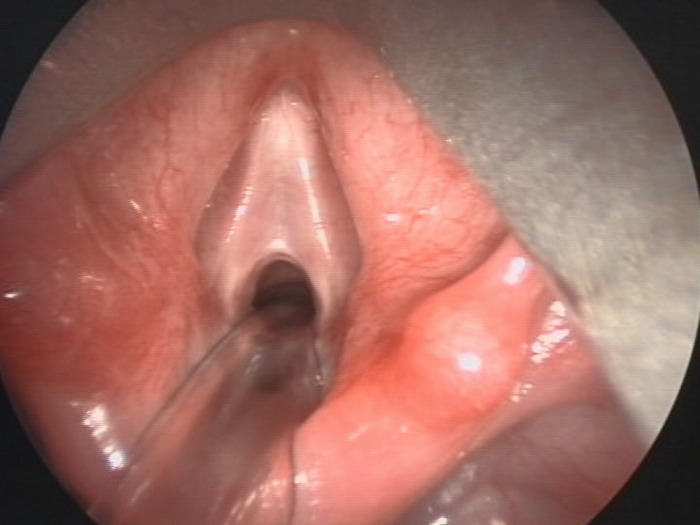
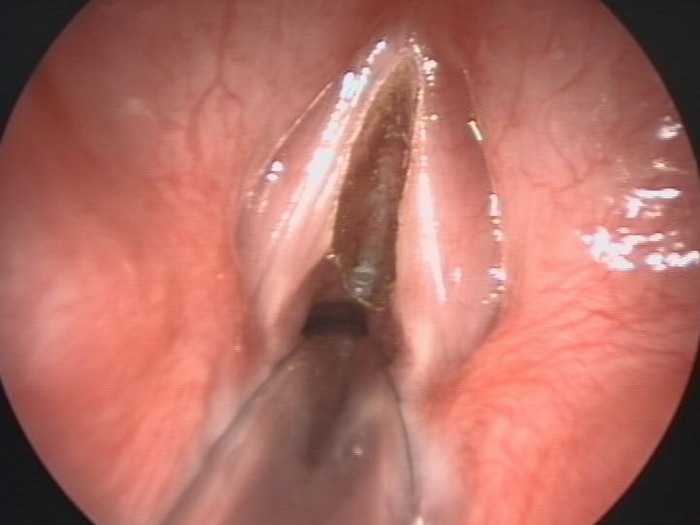
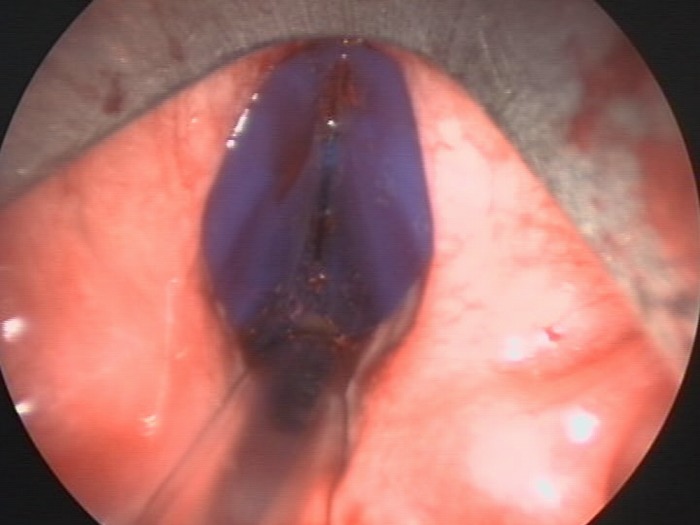
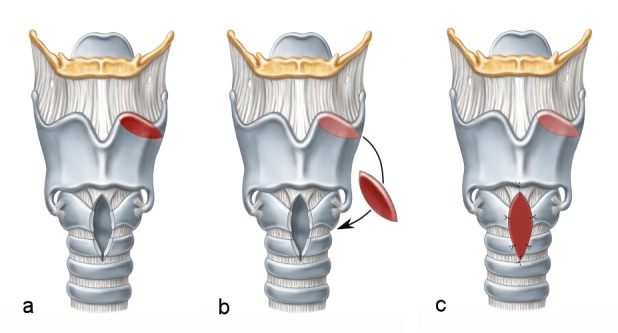
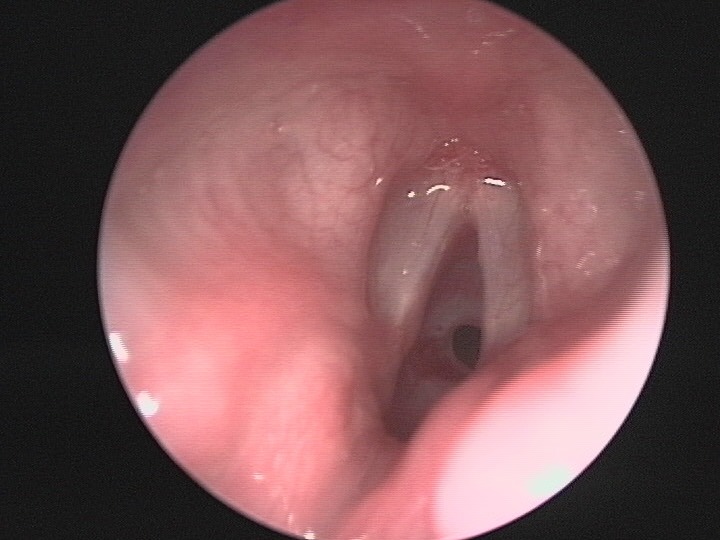
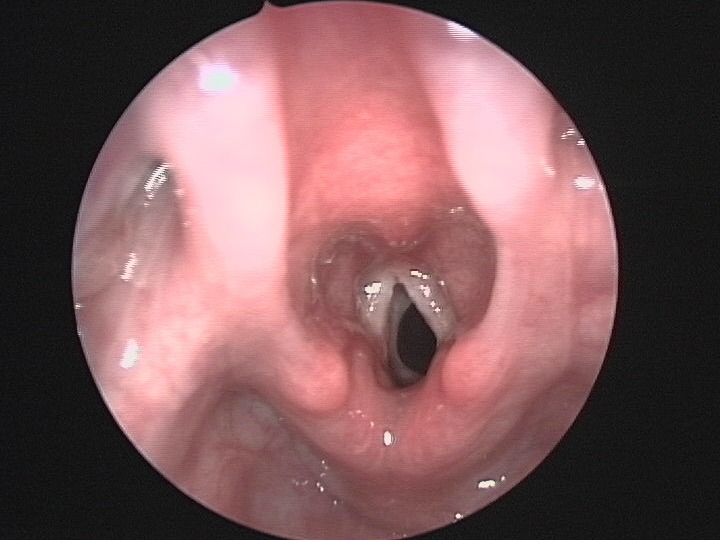
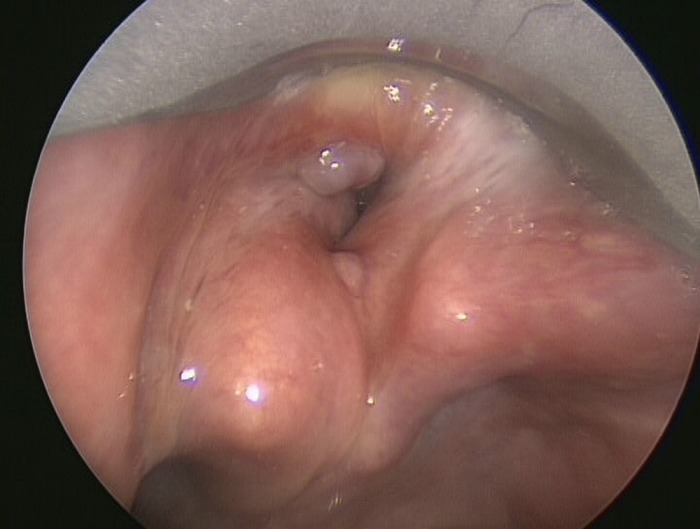
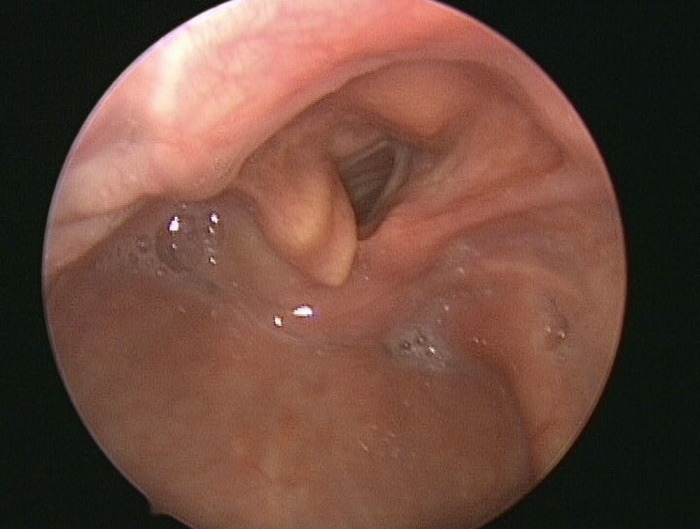
Pathologies in the larynx and trachea in the pediatric age can be characterized in 4 main groups: airway stenosis, acute infections, benign neoplasia and foreign body aspiration. In this review main diagnostic strategies and therapeutic options are presented. Laryngomalazia is the most frequent condition of supraglottic stenosis. The term supraglottoplasty summarizes all different techniques used for it's repair using an endoscopic approach. Glottic stenosis is rare in children. Usually a compromise between voice preservation and airway restoration has to be sought. Type of reconstruction and timing are varying considerably in individual cases, endoscopic approaches should be preferred. Subglottic stenosis remains the largest group in paediatric airway pathology, with cicatrial stenosis being predominant. Today, cricotracheal resection is the most successful treatment option, followed by the classical laryngotracheal reconstruction with autologous cartilage. In early infancy subglottic stenosis is particularly demanding. Endoscopic treatment is possible in selected patients, but open reconstruction is superior in more severe cases. Tracheostomy is not a safe airway in early infancy, it's indication should be strict. Foreign body aspiration needs to be managed according to a clear algorhythm. Recurrent respiratory papillomatosis should be treated with emphasis on function preservation. The role of adjuvant medication remains unclear. Infectious diseases can be managed conservatively by a pediatrician in the majority of cases.
Keywords: cricotracheal resection; laryngotracheal reconstruction; pediatric airway stenosis; pediatric subglottic stenosis.
Figures



References
-
- Berkowitz RG. Natural history of tracheostomy-dependent idiopathic congenital bilateral vocal fold paralysis. Otolaryngol Head Neck Surg. 2007 Apr;136(4):649–652. doi: 10.1016/j.otohns.2006.11.050. Available from: http://dx.doi.org/10.1016/j.otohns.2006.11.050. - DOI - DOI - PubMed
-
- Bielamowicz S, Villagomez V, Stager SV, Wilson WR. Intralesional cidofovir therapy for laryngeal papilloma in an adult cohort. Laryngoscope. 2002 Apr;112(4):696–699. doi: 10.1097/00005537-200204000-00019. Available from: http://dx.doi.org/10.1097/00005537-200204000-00019. - DOI - DOI - PubMed
-
- Carrat X, Verhulst J, Duroux S, Pescio P, Devars F, Traissac L. Postintubation interarytenoid adhesion. Ann Otol Rhinol Laryngol. 2000 Aug;109(8 Pt 1):736–740. - PubMed
-
- Chadha NK, James A. Adjuvant antiviral therapy for recurrent respiratory papillomatosis. Cochrane Database Syst Rev. 2012;12:CD005053. doi: 10.1002/14651858.CD005053.pub4. Available from: http://dx.doi.org/10.1002/14651858.CD005053.pub4. - DOI - DOI - PMC - PubMed
-
- Corbett HJ, Mann KS, Mitra I, Jesudason EC, Losty PD, Clarke RW. Tracheostomy--a 10-year experience from a UK pediatric surgical center. J Pediatr Surg. 2007 Jul;42(7):1251–1254. doi: 10.1016/j.jpedsurg.2007.02.017. Available from: http://dx.doi.org/10.1016/j.jpedsurg.2007.02.017. - DOI - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
