

Evaluation of antigen-specific immunoglobulin g responses in pulmonary tuberculosis patients and contacts
- PMID: 25588651
- PMCID: PMC4390664
- DOI: 10.1128/JCM.03050-14
Evaluation of antigen-specific immunoglobulin g responses in pulmonary tuberculosis patients and contacts
Abstract
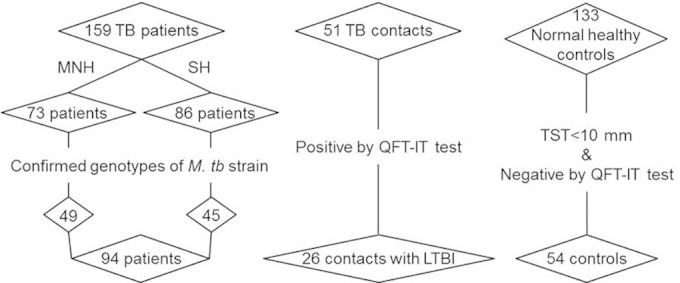
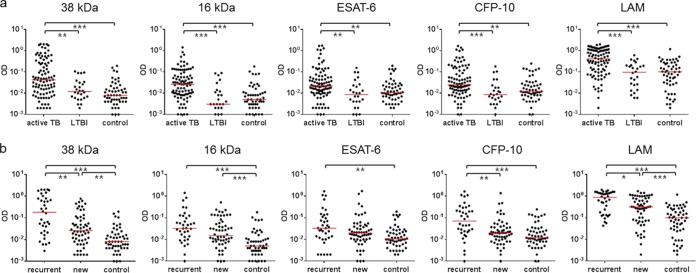
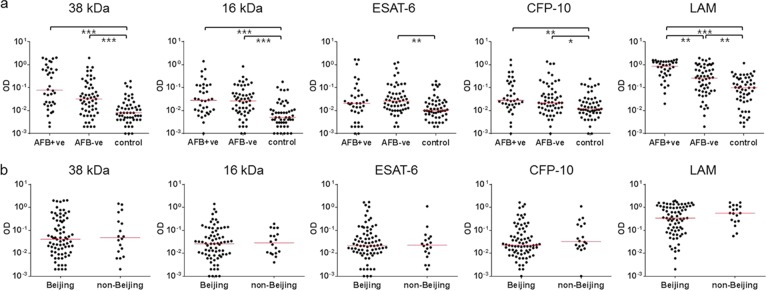
This study aimed to evaluate the serodiagnostic potential of immunoglobulin G (IgG) responses to Mycobacterium tuberculosis antigens in pulmonary tuberculosis (TB) patients, recent TB contacts with latent TB infection (LTBI), and healthy subjects. Infections were assessed using tuberculin skin tests, QuantiFERON-TB Gold In-Tube tests, drug susceptibility testing, and molecular genotyping of clinical isolates. Serum IgG responses to selective M. tuberculosis antigens, including the 38-kDa and 16-kDa antigens, lipoarabinomannan (LAM), and recombinant early secreted antigen target 6 kDa (ESAT-6) and culture filtrate protein 10 kDa (CFP-10), were determined. We found that the serum IgG responses to all antigens might differentiate between active TB and LTBI, with LAM having the highest diagnostic value (area under the curve [AUC] of 0.7756, P < 0.001). Recurrent TB cases showed significantly higher IgG responses to 38 kDa, CFP-10 (P < 0.01), and LAM (P < 0.05) than new cases, and male patients had higher levels of antigen-specific IgG than females (P < 0.05). Conversely, drug resistance and patient body mass index did not affect IgG responses (P > 0.05). LAM-specific IgG responses differentiated between acid-fast bacillus (AFB) smear-positive and -negative patients (P < 0.01), whereas antigen-specific IgG responses did not vary with the M. tuberculosis genotype (P > 0.05). Significantly higher IgG responses to 38 kDa and 16 kDa were observed in AFB smear-negative patients than in controls. These results suggest that assessment of serum IgG responses to selective purified M. tuberculosis antigens may help improve the diagnosis of active TB, particularly for sputum smear-negative patients or recurrent cases, and these may also help to differentiate between active TB and LTBI.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures

References
-
- World Health Organization. 2013. Global tuberculosis report 2013. http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf?ua=1.
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. 1999. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA 282:677–686. - PubMed
-
- World Health Organization. 2014. Multidrug-resistant tuberculosis (MDR-TB): 2014 update. http://www.who.int/tb/challenges/mdr/mdr_tb_factsheet.pdf.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
