

Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis: a multicentre, randomised, double-blind, non-inferiority trial versus celecoxib
- PMID: 25589511
- PMCID: PMC4717399
- DOI: 10.1136/annrheumdis-2014-206792
Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis: a multicentre, randomised, double-blind, non-inferiority trial versus celecoxib
Abstract
Objectives: To compare the efficacy and safety of chondroitin sulfate plus glucosamine hydrochloride (CS+GH) versus celecoxib in patients with knee osteoarthritis and severe pain.
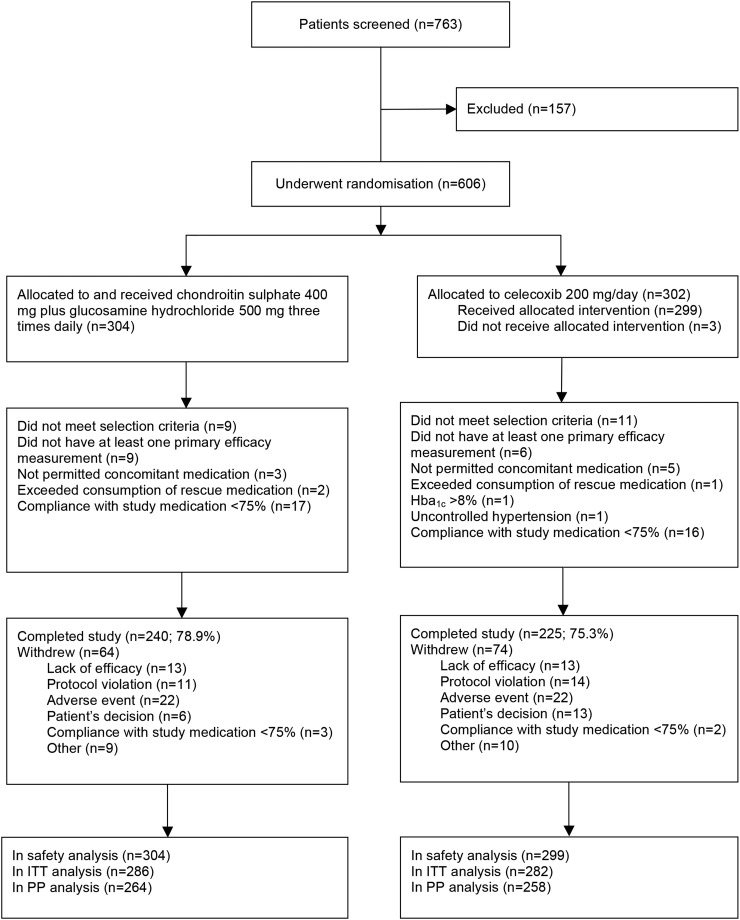
Methods: Double-blind Multicentre Osteoarthritis interVEntion trial with SYSADOA (MOVES) conducted in France, Germany, Poland and Spain evaluating treatment with CS+GH versus celecoxib in 606 patients with Kellgren and Lawrence grades 2-3 knee osteoarthritis and moderate-to-severe pain (Western Ontario and McMaster osteoarthritis index (WOMAC) score ≥301; 0-500 scale). Patients were randomised to receive 400 mg CS plus 500 mg GH three times a day or 200 mg celecoxib every day for 6 months. The primary outcome was the mean decrease in WOMAC pain from baseline to 6 months. Secondary outcomes included WOMAC function and stiffness, visual analogue scale for pain, presence of joint swelling/effusion, rescue medication consumption, Outcome Measures in Rheumatology Clinical Trials and Osteoarthritis Research Society International (OMERACT-OARSI) criteria and EuroQoL-5D.
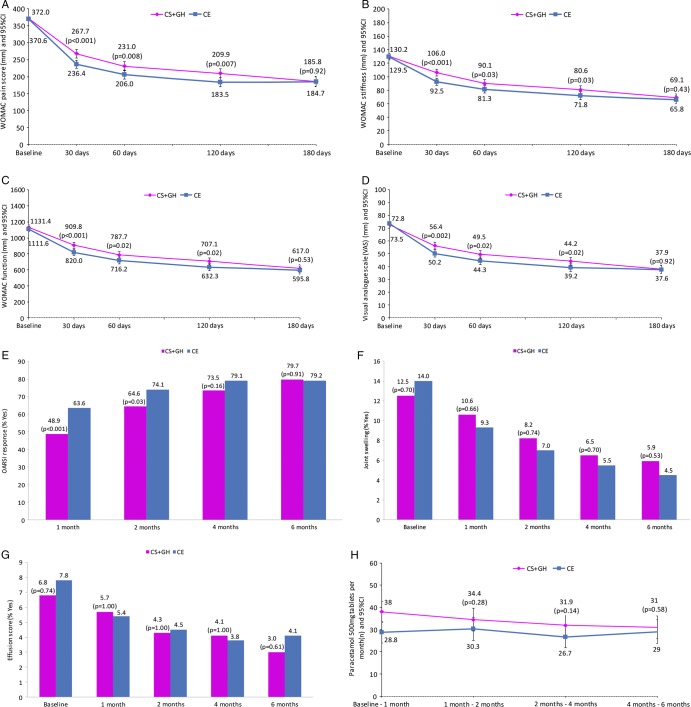
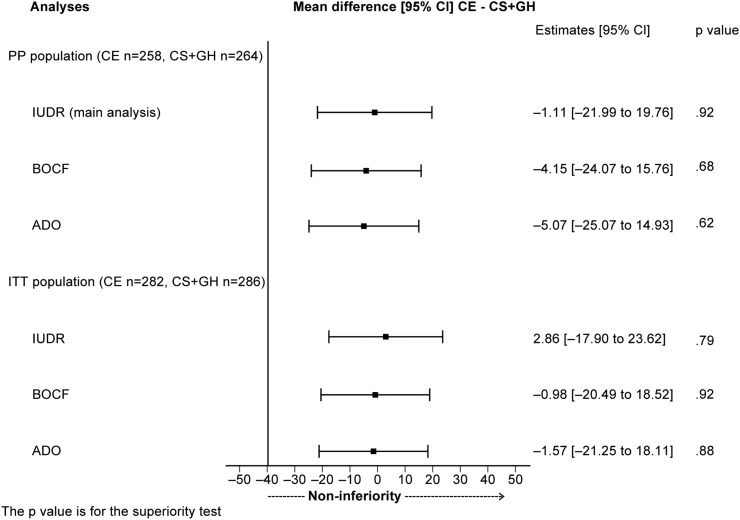
Results: The adjusted mean change (95% CI) in WOMAC pain was -185.7 (-200.3 to -171.1) (50.1% decrease) with CS+GH and -186.8 (-201.7 to -171.9) (50.2% decrease) with celecoxib, meeting the non-inferiority margin of -40: -1.11 (-22.0 to 19.8; p=0.92). All sensitivity analyses were consistent with that result. At 6 months, 79.7% of patients in the combination group and 79.2% in the celecoxib group fulfilled OMERACT-OARSI criteria. Both groups elicited a reduction >50% in the presence of joint swelling; a similar reduction was seen for effusion. No differences were observed for the other secondary outcomes. Adverse events were low and similarly distributed between groups.
Conclusions: CS+GH has comparable efficacy to celecoxib in reducing pain, stiffness, functional limitation and joint swelling/effusion after 6 months in patients with painful knee osteoarthritis, with a good safety profile.
Trial registration number: NCT01425853.
Keywords: Analgesics; NSAIDs; Osteoarthritis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Comment in
-
Clinical trials: Glucosamine-chondroitin combo improves knee OA pain.Nat Rev Rheumatol. 2015 Mar;11(3):126. doi: 10.1038/nrrheum.2015.9. Epub 2015 Feb 3. Nat Rev Rheumatol. 2015. PMID: 25644053 No abstract available.
References
-
- Smalley WE, Ray WA, Daugherty JR, et al. . Nonsteroidal anti-inflammatory drugs and the incidence of hospitalizations for peptic ulcer disease in elderly persons. Am J Epidemiol 1995;141:539–45. - PubMed
-
- Coxib and traditional NSAID Trialists' (CNT) Collaboration, Bhala N, Emberson J, Merhi A, et al Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet 2013;382:769–79. 10.1016/S0140-6736(13)60900-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
