

Diagnosis and Prediction of CKD Progression by Assessment of Urinary Peptides
- PMID: 25589610
- PMCID: PMC4520165
- DOI: 10.1681/ASN.2014050423
Diagnosis and Prediction of CKD Progression by Assessment of Urinary Peptides
Abstract
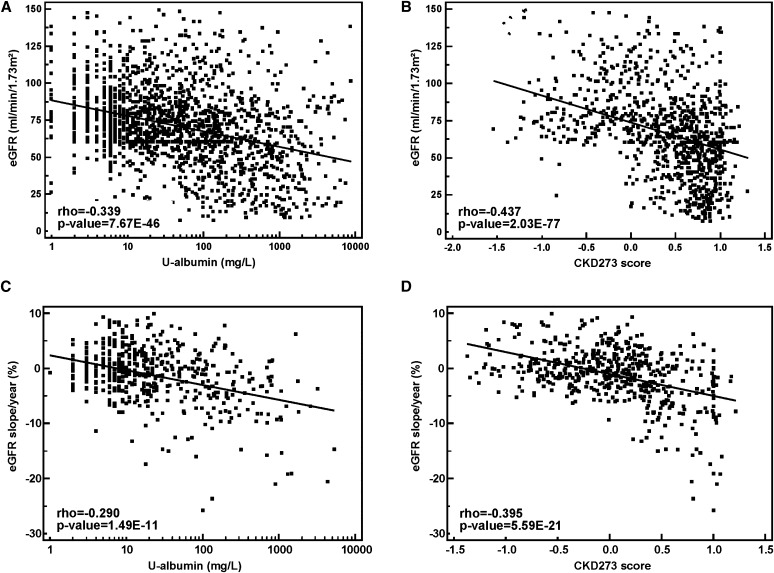
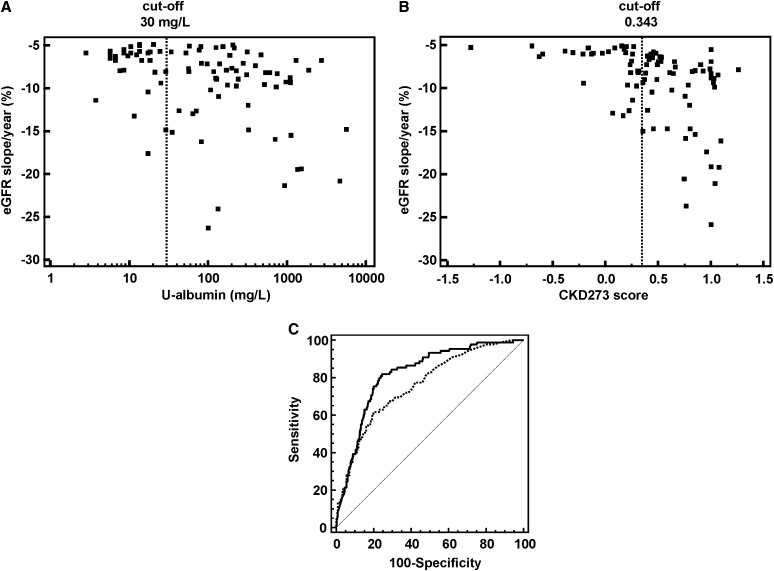
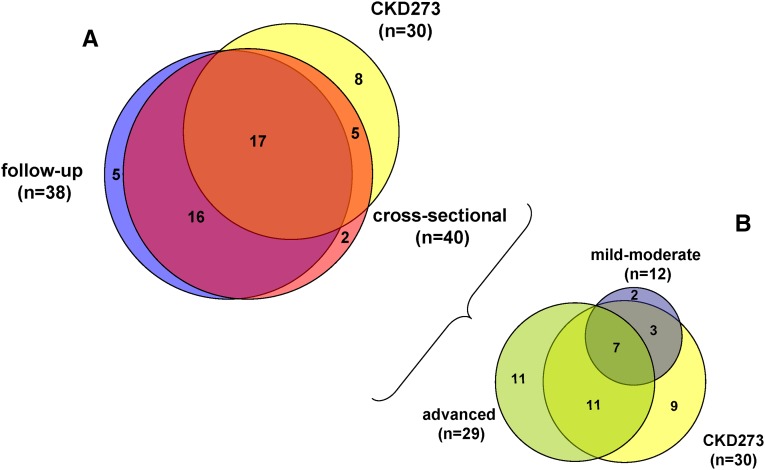
Progressive CKD is generally detected at a late stage by a sustained decline in eGFR and/or the presence of significant albuminuria. With the aim of early and improved risk stratification of patients with CKD, we studied urinary peptides in a large cross-sectional multicenter cohort of 1990 individuals, including 522 with follow-up data, using proteome analysis. We validated that a previously established multipeptide urinary biomarker classifier performed significantly better in detecting and predicting progression of CKD than the current clinical standard, urinary albumin. The classifier was also more sensitive for identifying patients with rapidly progressing CKD. Compared with the combination of baseline eGFR and albuminuria (area under the curve [AUC]=0.758), the addition of the multipeptide biomarker classifier significantly improved CKD risk prediction (AUC=0.831) as assessed by the net reclassification index (0.303±-0.065; P<0.001) and integrated discrimination improvement (0.058±0.014; P<0.001). Correlation of individual urinary peptides with CKD stage and progression showed that the peptides that associated with CKD, irrespective of CKD stage or CKD progression, were either fragments of the major circulating proteins, suggesting failure of the glomerular filtration barrier sieving properties, or different collagen fragments, suggesting accumulation of intrarenal extracellular matrix. Furthermore, protein fragments associated with progression of CKD originated mostly from proteins related to inflammation and tissue repair. Results of this study suggest that urinary proteome analysis might significantly improve the current state of the art of CKD detection and outcome prediction and that identification of the urinary peptides allows insight into various ongoing pathophysiologic processes in CKD.
Keywords: CKD; albuminuria; biomarker; extracellular matrix; fibrosis; renal progression.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Can the Urinary Peptidome Outperform Creatinine and Albumin to Predict Renal Function Decline?J Am Soc Nephrol. 2015 Aug;26(8):1760-1. doi: 10.1681/ASN.2014121243. Epub 2015 Jan 14. J Am Soc Nephrol. 2015. PMID: 25589613 Free PMC article. No abstract available.
Similar articles
-
A urinary proteome-based classifier for the early detection of decline in glomerular filtration.Nephrol Dial Transplant. 2017 Sep 1;32(9):1510-1516. doi: 10.1093/ndt/gfw239. Nephrol Dial Transplant. 2017. PMID: 27387473
-
Novel Urinary Biomarkers For Improved Prediction Of Progressive Egfr Loss In Early Chronic Kidney Disease Stages And In High Risk Individuals Without Chronic Kidney Disease.Sci Rep. 2018 Oct 29;8(1):15940. doi: 10.1038/s41598-018-34386-8. Sci Rep. 2018. PMID: 30374033 Free PMC article.
-
Dickkopf-3 (DKK3) in Urine Identifies Patients with Short-Term Risk of eGFR Loss.J Am Soc Nephrol. 2018 Nov;29(11):2722-2733. doi: 10.1681/ASN.2018040405. Epub 2018 Oct 2. J Am Soc Nephrol. 2018. PMID: 30279273 Free PMC article. Clinical Trial.
-
Utility of the CKD273 peptide classifier in predicting chronic kidney disease progression.Nephrol Dial Transplant. 2016 Feb;31(2):249-54. doi: 10.1093/ndt/gfv062. Epub 2015 Mar 19. Nephrol Dial Transplant. 2016. PMID: 25791724
-
Urinary neutrophil gelatinase-associated lipocalin may aid prediction of renal decline in patients with non-proteinuric Stages 3 and 4 chronic kidney disease (CKD).Nephrol Dial Transplant. 2013 Jun;28(6):1569-79. doi: 10.1093/ndt/gfs586. Epub 2013 Jan 16. Nephrol Dial Transplant. 2013. PMID: 23328709
Cited by
-
Proteomic characterization of obesity-related nephropathy.Clin Kidney J. 2020 Apr 15;13(4):684-692. doi: 10.1093/ckj/sfaa016. eCollection 2020 Aug. Clin Kidney J. 2020. PMID: 32905225 Free PMC article.
-
A urinary peptidomic profile predicts outcome in SARS-CoV-2-infected patients.EClinicalMedicine. 2021 Jun;36:100883. doi: 10.1016/j.eclinm.2021.100883. Epub 2021 May 3. EClinicalMedicine. 2021. PMID: 33969282 Free PMC article.
-
Urinary peptidomics reveals proteases involved in idiopathic membranous nephropathy.BMC Genomics. 2021 Nov 24;22(1):852. doi: 10.1186/s12864-021-08155-3. BMC Genomics. 2021. PMID: 34819020 Free PMC article.
-
OMICS in Chronic Kidney Disease: Focus on Prognosis and Prediction.Int J Mol Sci. 2021 Dec 29;23(1):336. doi: 10.3390/ijms23010336. Int J Mol Sci. 2021. PMID: 35008760 Free PMC article. Review.
-
Unmet medical needs in lupus nephritis: solutions through evidence-based, personalized medicine.Clin Kidney J. 2015 Oct;8(5):492-502. doi: 10.1093/ckj/sfv072. Epub 2015 Aug 27. Clin Kidney J. 2015. PMID: 26413272 Free PMC article.
References
-
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, Saran R, Wang AY, Yang CW: Chronic kidney disease: Global dimension and perspectives. Lancet 382: 260–272, 2013 - PubMed
-
- O’Hare AM, Choi AI, Bertenthal D, Bacchetti P, Garg AX, Kaufman JS, Walter LC, Mehta KM, Steinman MA, Allon M, McClellan WM, Landefeld CS: Age affects outcomes in chronic kidney disease. J Am Soc Nephrol 18: 2758–2765, 2007 - PubMed
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX: Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 17: 2034–2047, 2006 - PubMed
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, Nahas ME, Jaber BL, Jadoul M, Levin A, Powe NR, Rossert J, Wheeler DC, Lameire N, Eknoyan G: Chronic kidney disease as a global public health problem: Approaches and initiatives - A position statement from Kidney Disease Improving Global Outcomes. Kidney Int 72: 247–259, 2007 - PubMed
-
- Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, De Zeeuw D, Hostetter TH, Lameire N, Eknoyan G: Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 67: 2089–2100, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
