Effect of cause-of-death training on agreement between hospital discharge diagnoses and cause of death reported, inpatient hospital deaths, New York City, 2008-2010
- PMID: 25590598
- PMCID: PMC4307833
- DOI: 10.5888/pcd12.140299
Effect of cause-of-death training on agreement between hospital discharge diagnoses and cause of death reported, inpatient hospital deaths, New York City, 2008-2010
Abstract
Introduction: Accurate cause-of-death reporting is required for mortality data to validly inform public health programming and evaluation. Research demonstrates overreporting of heart disease on New York City death certificates. We describe changes in reported causes of death following a New York City health department training conducted in 2009 to improve accuracy of cause-of-death reporting at 8 hospitals. The objective of our study was to assess the degree to which death certificates citing heart disease as cause of death agreed with hospital discharge data and the degree to which training improved accuracy of reporting.
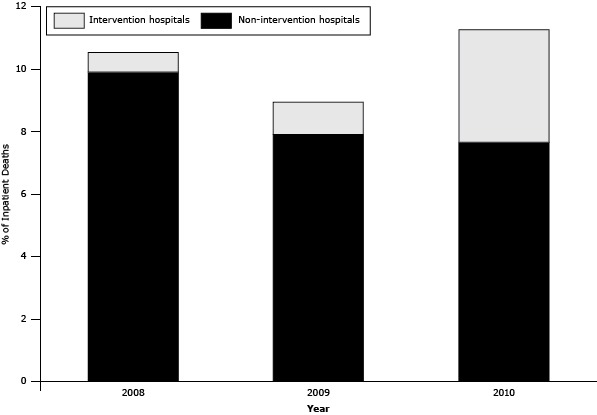
Methods: We analyzed 74,373 death certificates for 2008 through 2010 that were linked with hospital discharge records for New York City inpatient deaths and calculated the proportion of discordant deaths, that is, death certificates reporting an underlying cause of heart disease with no corresponding discharge record diagnosis. We also summarized top principal diagnoses among discordant reports and calculated the proportion of inpatient deaths reporting sepsis, a condition underreported in New York City, to assess whether documentation practices changed in response to clarifications made during the intervention.
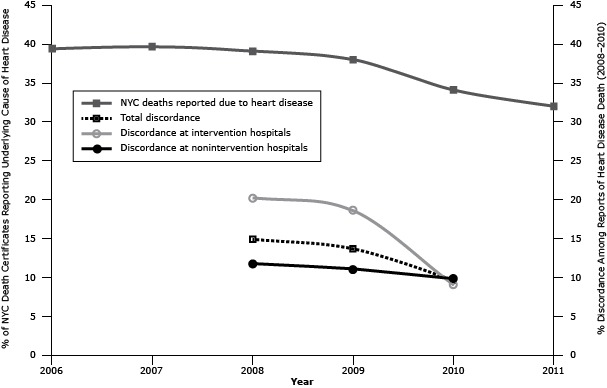
Results: Citywide discordance between death certificates and discharge data decreased from 14.9% in 2008 to 9.6% in 2010 (P < .001), driven by a decrease in discordance at intervention hospitals (20.2% in 2008 to 8.9% in 2010; P < .001). At intervention hospitals, reporting of sepsis increased from 3.7% of inpatient deaths in 2008 to 20.6% in 2010 (P < .001).
Conclusion: Overreporting of heart disease as cause of death declined at intervention hospitals, driving a citywide decline, and sepsis reporting practices changed in accordance with health department training. Researchers should consider the effect of overreporting and data-quality changes when analyzing New York City heart disease mortality trends. Other vital records jurisdictions should employ similar interventions to improve cause-of-death reporting and use linked discharge data to monitor data quality.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical