

Relationship between tumor size and survival in non-small-cell lung cancer (NSCLC): an analysis of the surveillance, epidemiology, and end results (SEER) registry
- PMID: 25590605
- PMCID: PMC4368494
- DOI: 10.1097/JTO.0000000000000456
Relationship between tumor size and survival in non-small-cell lung cancer (NSCLC): an analysis of the surveillance, epidemiology, and end results (SEER) registry
Abstract
Introduction: Tumor size is a known prognostic factor for early stage non-small-cell lung cancer (NSCLC), but its significance in node-positive and locally invasive NSCLC has not been extensively characterized. We queried the Surveillance, Epidemiology, and End Results database to evaluate the prognostic value of tumor size for early stage and node-positive and locally invasive NSCLC.
Methods: Patients in Surveillance, Epidemiology, and End Results registry with NSCLC diagnosed between 1998 and 2003 were analyzed. Tumor size was analyzed as a continuous variable. Other demographic variables included age, gender, race, histology, primary tumor extension, node status, and primary treatment modality (surgery vs. radiation). The Kaplan-Meier method was used to estimate overall survival (OS). Cox proportional hazard model was used to evaluate whether tumor size was an independent prognostic factor.
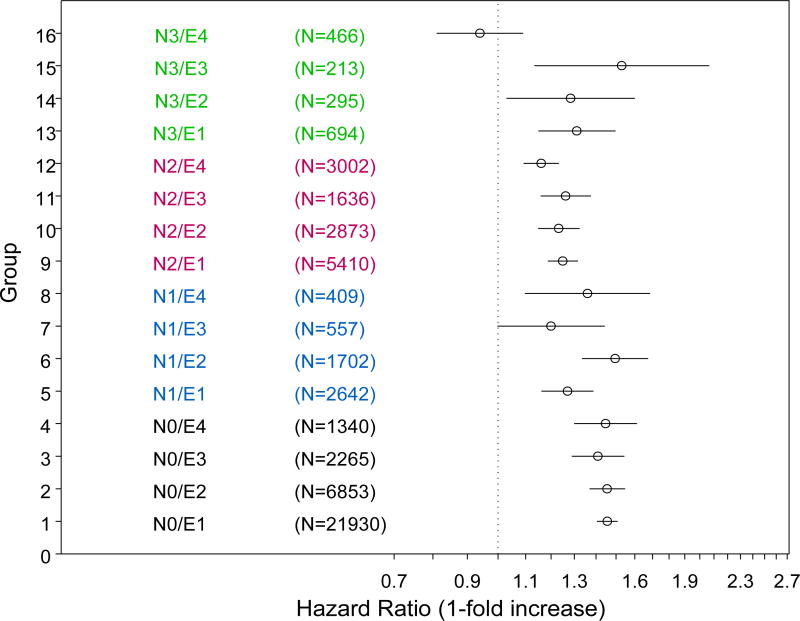
Results: In all, 52,287 eligible patients were subgrouped based on tumor extension and node status. Tumor size had a significant effect on OS in all subgroups defined by tumor extension or node status. In addition, tumor size also had statistically significant effect on OS in 15 of 16 subgroups defined by tumor extension and nodal status after adjustment for other clinical variables. Our model incorporating tumor size had significantly better predictive accuracy than our alternative model without tumor size.
Conclusions: Tumor size is an independent prognostic factor, for early stage and node-positive and locally invasive disease. Prediction tools, such as nomograms, incorporating more detailed information not captured in detail by the routine tumor, node, metastasis classification, may improve prediction accuracy of OS in NSCLC.
Figures




References
-
- Motta G, Carbone E, Spinelli E, et al. Considerations about tumor size as a factor of prognosis in NSCLC. Ann Ital Chir. 1999;70:893–7. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–14. - PubMed
-
- Groome PA, Bolejack V, Crowley JJ, et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:694–705. - PubMed
-
- Postmus PE, Brambilla E, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for revision of the M descriptors in the forthcoming (seventh) edition of the TNM classification of lung cancer. J Thorac Oncol. 2007;2:686–93. - PubMed
-
- Rami-Porta R, Ball D, Crowley J, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the T descriptors in the forthcoming (seventh) edition of the TNM classification for lung cancer. J Thorac Oncol. 2007;2:593–602. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
