

Age-adjusted Charlson comorbidity index scores as predictor of survival in colorectal cancer patients who underwent surgical resection and chemoradiation
- PMID: 25590852
- PMCID: PMC4602551
- DOI: 10.1097/MD.0000000000000431
Age-adjusted Charlson comorbidity index scores as predictor of survival in colorectal cancer patients who underwent surgical resection and chemoradiation
Abstract
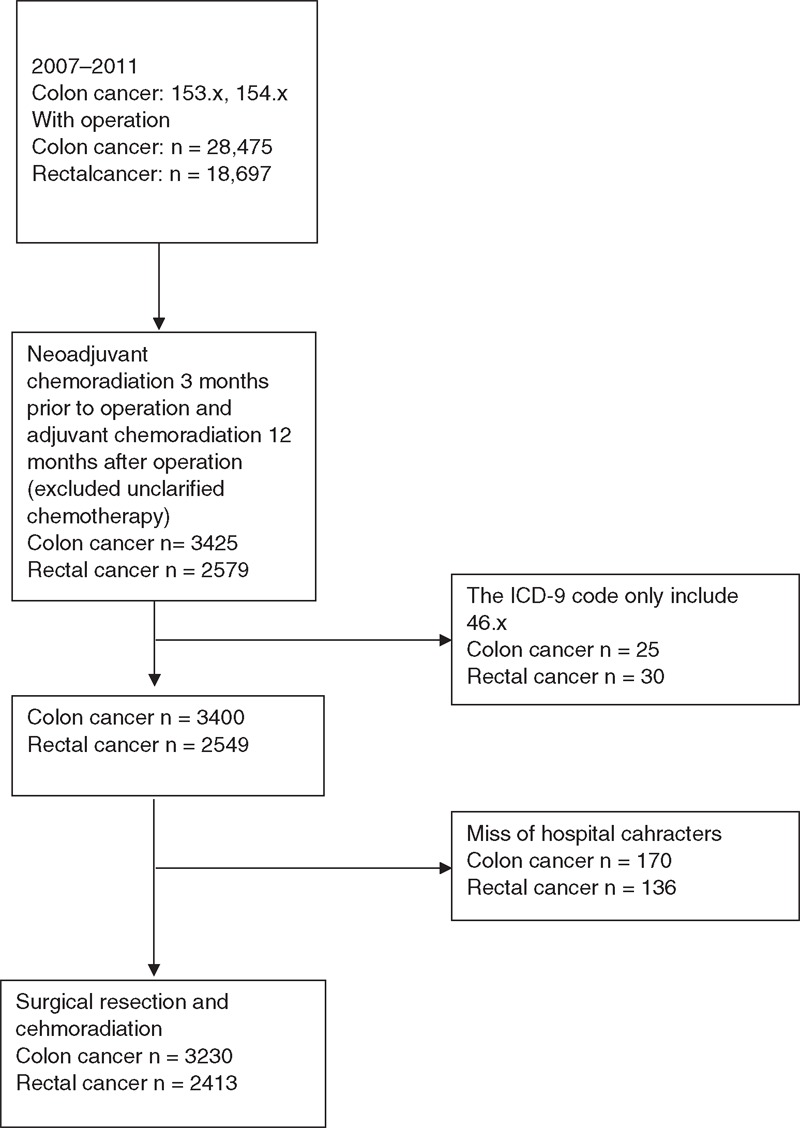
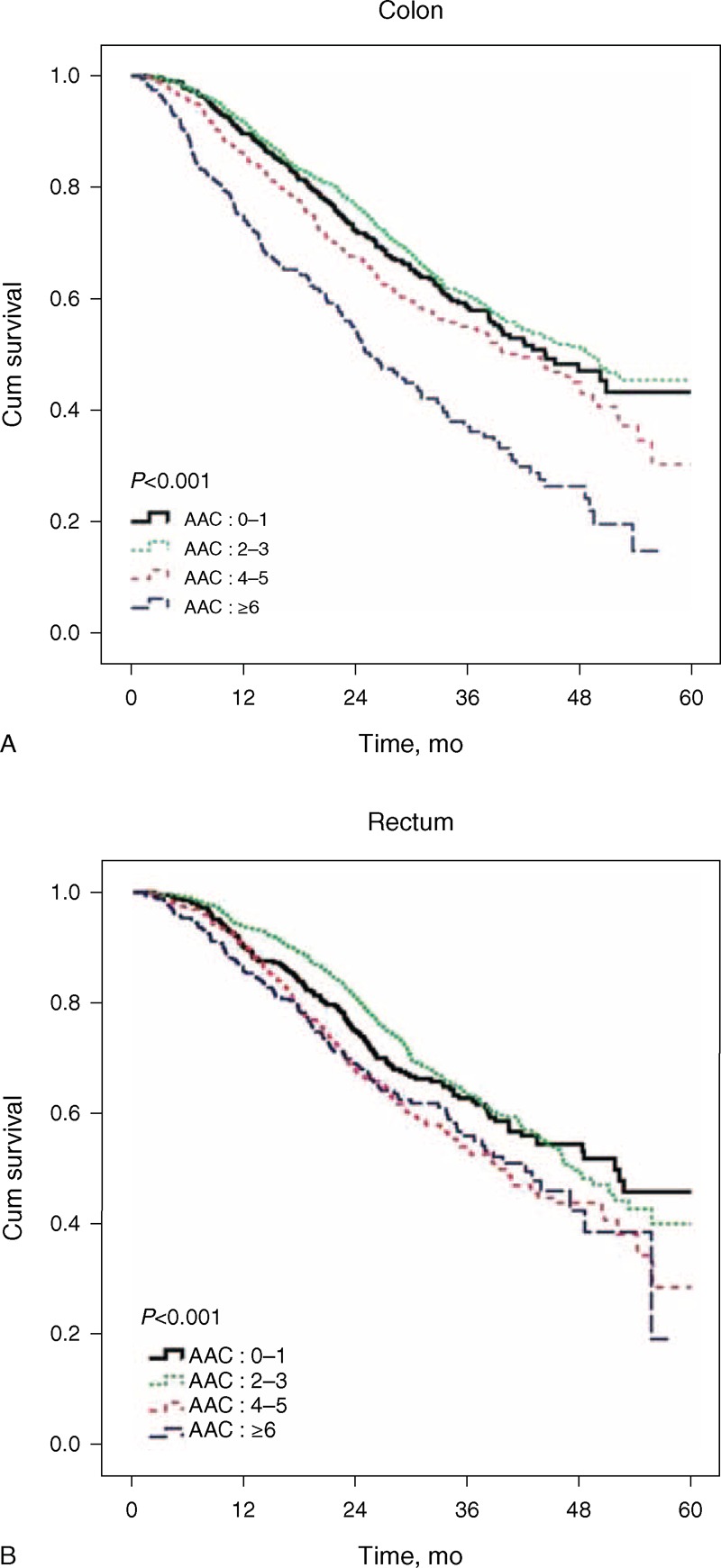
We studied the effect of Age-Adjusted Comorbidity Index Score in colorectal cancer patients who underwent similarly aggressive treatment. Using the National Health Insurance Research Database of Taiwan, we identified 5643 patients with colorectal cancer who underwent surgical resection and chemoradiation from 2007 through 2011. We estimated survival according to Age-Adjusted Comorbidity Index Scores and 5-year survival using Cox proportional hazard regression analysis, adjusting for sex, oxaliplatin-based chemotherapy, socioeconomic status, geographic region, and hospital characteristics. In the cohort were 3230 patients with colonic cancer and 2413 patients with rectal cancer, who had undergone combined surgical resection and either neoadjuvant or adjuvant chemoradiation. After adjusting for patient characteristics (sex, oxaliplatin-based chemotherapy, socioeconomic status, geographic region, and hospital-characteristics), colonic cancer patients with age-adjusted Charlson (AAC) ≥ 6 had a 106% greater risk of death within 5 years (adjusted HR = 2.06; 95% CI, 1.66-2.56). In rectal cancer patients, patients with an AAC score of 4-5 had a 28% greater risk of death within 5 years (adjusted HR = 1.28; 95% CI, 1.02-1.61), and those with AAC ≥ 6 had a 47% greater risk (adjusted HR = 1.47; 95% CI, 1.15-1.90). Age and burden of comorbidities influence survival of patients with colonic or rectal cancer. Age-Adjusted Comorbidity Score remains an independent prognostic factor even after adjusting for the aggressiveness of treatment.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010; 127:2893–2917. - PubMed
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69–90. - PubMed
-
- van Leersum NJ, Janssen-Heijnen ML, Wouters MW, et al. Increasing prevalence of comorbidity in patients with colorectal cancer in the South of the Netherlands 1995-2010. Int J Cancer 2013; 132:2157–2163. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
