

Biologic concentration testing in inflammatory bowel disease
- PMID: 25590953
- PMCID: PMC4437804
- DOI: 10.1097/MIB.0000000000000312
Biologic concentration testing in inflammatory bowel disease
Abstract
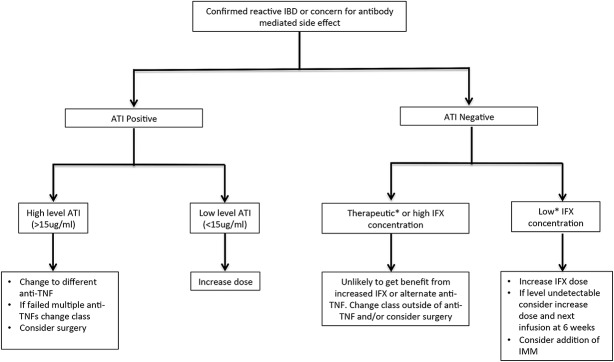
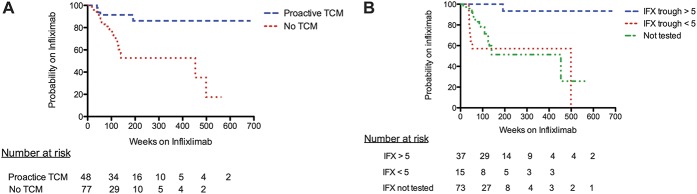
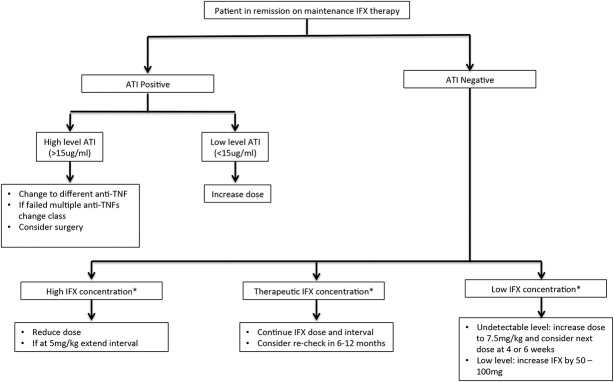
Anti-TNF medications have revolutionized the care of patients with inflammatory bowel disease. However, despite an initial robust effect, loss of response is common and long-term results are disappointing. Much of this lack of durability may be due to inadequate dose optimization, and recent studies suggest a correlation between serum drug concentrations and clinical outcomes. Currently, in clinical practice, measurement of drug concentrations and antibodies to drug are typically performed only when a patient presents with active inflammatory bowel disease symptoms or during a potential immune-mediated reaction to anti-TNF ("reactive" setting). However, proactive monitoring of anti-TNF concentrations with titration to a therapeutic window (i.e., therapeutic concentration monitoring) represents a new strategy with many potential clinical benefits including prevention of immunogenicity, less need for IFX rescue therapy, and greater durability of IFX treatment. This review will cover the salient features of anti-TNF pharmacokinetics and pharmacodynamics and provide a rational approach for the use of anti-TNF concentration testing in both the reactive and proactive settings.
Conflict of interest statement
W. J. Sandborn has consulted for Prometheus and Janssen and has research support from Janssen. A. S. Cheifetz has consulted for or participated in advisory boards for Prometheus, Janssen, Abbvie, Takeda and research support from Pfizer. The remaining author has no conflicts of interest to disclose.
Figures
References
-
- Danese S, Fiorino G, Reinisch W. Review article: causative factors and the clinical management of patients with Crohn's disease who lose response to anti-TNF-alpha therapy. Aliment Pharmacol Ther. 2011;34:1–10. - PubMed
-
- Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn's disease. N Engl J Med. 2010;362:1383–1395. - PubMed
-
- Imaeda H, Bamba S, Takahashi K, et al. Relationship between serum infliximab trough levels and endoscopic activities in patients with Crohn's disease under scheduled maintenance treatment. J Gastroenterol. 2014;49:674–682. - PubMed
-
- Karmiris K, Paintaud G, Noman M, et al. Influence of trough serum levels and immunogenicity on long-term outcome of adalimumab therapy in Crohn's disease. Gastroenterology. 2009;137:1628–1640. - PubMed
