

Sulphadoxine-pyrimethamine plus azithromycin for the prevention of low birthweight in Papua New Guinea: a randomised controlled trial
- PMID: 25591391
- PMCID: PMC4305224
- DOI: 10.1186/s12916-014-0258-3
Sulphadoxine-pyrimethamine plus azithromycin for the prevention of low birthweight in Papua New Guinea: a randomised controlled trial
Abstract
Background: Intermittent preventive treatment in pregnancy has not been evaluated outside of Africa. Low birthweight (LBW, <2,500 g) is common in Papua New Guinea (PNG) and contributing factors include malaria and reproductive tract infections.
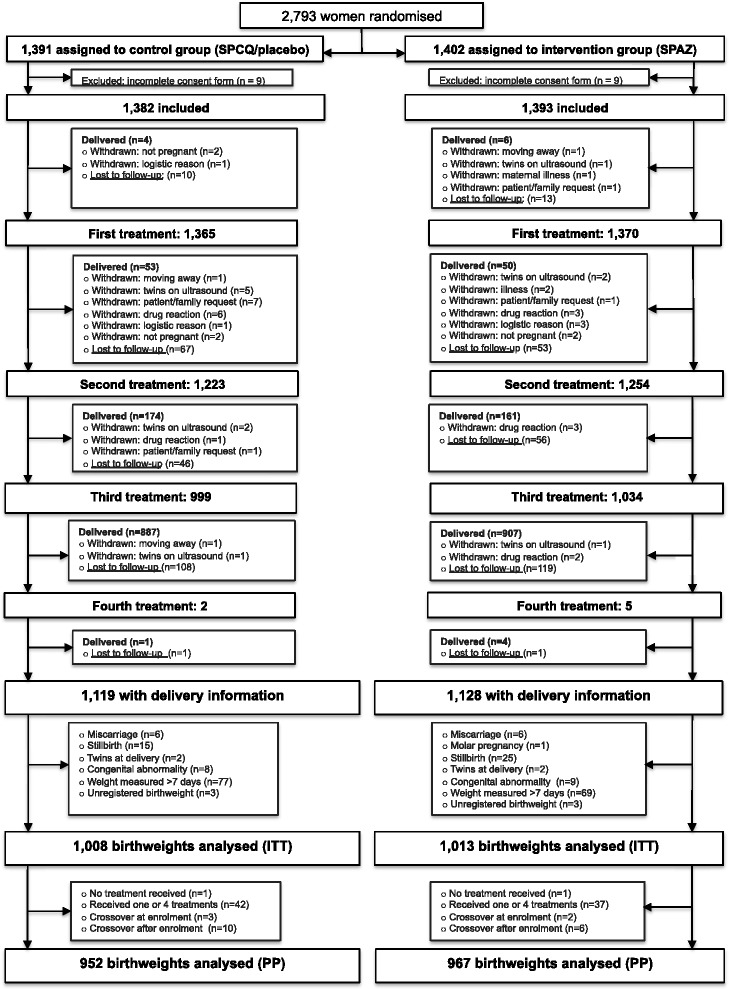
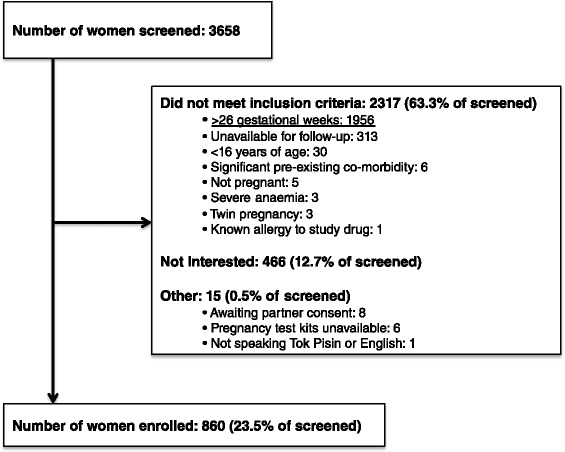
Methods: From November 2009 to February 2013, we conducted a parallel group, randomised controlled trial in pregnant women (≤ 26 gestational weeks) in PNG. Sulphadoxine-pyrimethamine (1,500/75 mg) plus azithromycin (1 g twice daily for 2 days) (SPAZ) monthly from second trimester (intervention) was compared against sulphadoxine-pyrimethamine and chloroquine (450 to 600 mg, daily for three days) (SPCQ) given once, followed by SPCQ placebo (control). Women were assigned to treatment (1:1) using a randomisation sequence with block sizes of 32. Participants were blinded to assignments. The primary outcome was LBW. Analysis was by intention-to-treat.
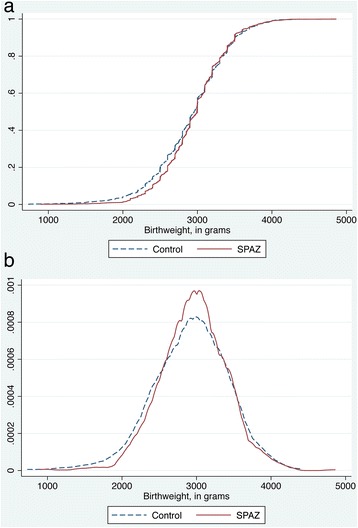
Results: Of 2,793 women randomised, 2,021 (72.4%) were included in the primary outcome analysis (SPCQ: 1,008; SPAZ: 1,013). The prevalence of LBW was 15.1% (305/2,021). SPAZ reduced LBW (risk ratio [RR]: 0.74, 95% CI: 0.60-0.91, P = 0.005; absolute risk reduction (ARR): 4.5%, 95% CI: 1.4-7.6; number needed to treat: 22), and preterm delivery (0.62, 95% CI: 0.43-0.89, P = 0.010), and increased mean birthweight (41.9 g, 95% CI: 0.2-83.6, P = 0.049). SPAZ reduced maternal parasitaemia (RR: 0.57, 95% CI: 0.35-0.95, P = 0.029) and active placental malaria (0.68, 95% CI: 0.47-0.98, P = 0.037), and reduced carriage of gonorrhoea (0.66, 95% CI: 0.44-0.99, P = 0.041) at second visit. There were no treatment-related serious adverse events (SAEs), and the number of SAEs (intervention 13.1% [181/1,378], control 12.7% [174/1,374], P = 0.712) and AEs (intervention 10.5% [144/1,378], control 10.8% [149/1,374], P = 0.737) was similar. A major limitation of the study was the high loss to follow-up for birthweight.
Conclusions: SPAZ was efficacious and safe in reducing LBW, possibly acting through multiple mechanisms including the effect on malaria and on sexually transmitted infections. The efficacy of SPAZ in the presence of resistant parasites and the contribution of AZ to bacterial antibiotic resistance require further study. The ability of SPAZ to improve pregnancy outcomes warrants further evaluation.
Trial registration: ClinicalTrials.gov NCT01136850 (06 April 2010).
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
