

Caffeine intake from food and beverage sources and trends among children and adolescents in the United States: review of national quantitative studies from 1999 to 2011
- PMID: 25593149
- PMCID: PMC4288269
- DOI: 10.3945/an.114.007401
Caffeine intake from food and beverage sources and trends among children and adolescents in the United States: review of national quantitative studies from 1999 to 2011
Abstract
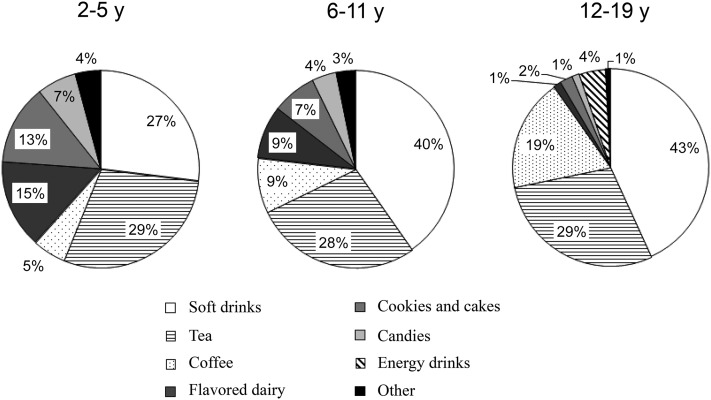
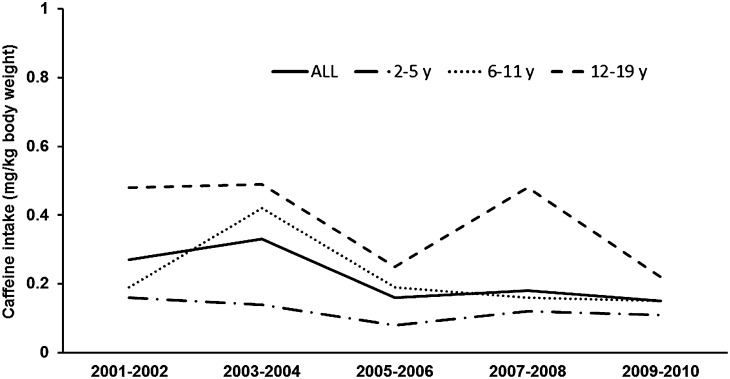
There is increasing concern about potential adverse effects of caffeine in children. Our understanding of caffeine intake relies on studies dating to the late 1990s. This article synthesizes information from national studies since then to describe caffeine consumption, its association with sociodemographic factors, key dietary sources including caffeine-containing energy drinks (CCEDs), and trends in caffeine intake and sources among US children. Findings from the Kanter Worldpanel (KWP) Beverage Consumption Panel and the NHANES showed that caffeine consumption prevalence was generally consistent across studies and over time; more than one-half of 2- to 5-y-olds and ∼75% of older children (>5 y) consumed caffeine. The usual intakes of caffeine were 25 and 50 mg/d for children and adolescents aged 2-11 and 12-17 y, respectively (NHANES 2007-2010). Caffeine consumption correlated with age and was higher in non-Hispanic white children. The key sources of caffeine were soda and tea as well as flavored dairy (for children aged <12 y) and coffee (for those aged ≥12 y). The frequency of CCED use varied (2-30%) depending on study setting, methods, and demographic characteristics. A statistically significant but small decline in caffeine intake was noted in children overall during the 10- to 12-y period examined; intakes remained stable among older children (≥12 y). A significant increasing trend in CCED and coffee consumption and a decline in soda intake were noted (1999-2010). In 2009-2010, 10% of 12- to 19-y-olds and 10-25% of caffeine consumers (aged 12-19 y) had intakes exceeding Canadian maximal guidelines. Continued monitoring can help better understand changes in caffeine consumption patterns of youth.
Keywords: adolescents; caffeine intake; children; dietary sources; trends.
© 2015 American Society for Nutrition.
Conflict of interest statement
Author disclosures: N Ahluwalia and K Herrick, no conflicts of interest.
Figures
References
-
- Barone JJ, Roberts HR. Caffeine consumption. Food Chem Toxicol 1996;34:119–29. - PubMed
-
- Heckman MA, Weil J, Gonzalez de Mejia E. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci 2010;75:R77–87. - PubMed
-
- Temple JL, Dewey AM, Briatico LN. Effects of acute caffeine administration on adolescents. Exp Clin Psychopharmacol 2010;18:510–20. - PubMed
-
- De Bellis MD, Keshavan MS, Beers SR, Hall J, Frustaci K, Masaledhan A, Noll J, Boring AM. Sex differences in brain maturation during childhood and adolescence. Cereb Cortex 2001;11:552–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
