

Composite end point of graft-versus-host disease-free, relapse-free survival after allogeneic hematopoietic cell transplantation
- PMID: 25593335
- PMCID: PMC4335084
- DOI: 10.1182/blood-2014-10-609032
Composite end point of graft-versus-host disease-free, relapse-free survival after allogeneic hematopoietic cell transplantation
Abstract
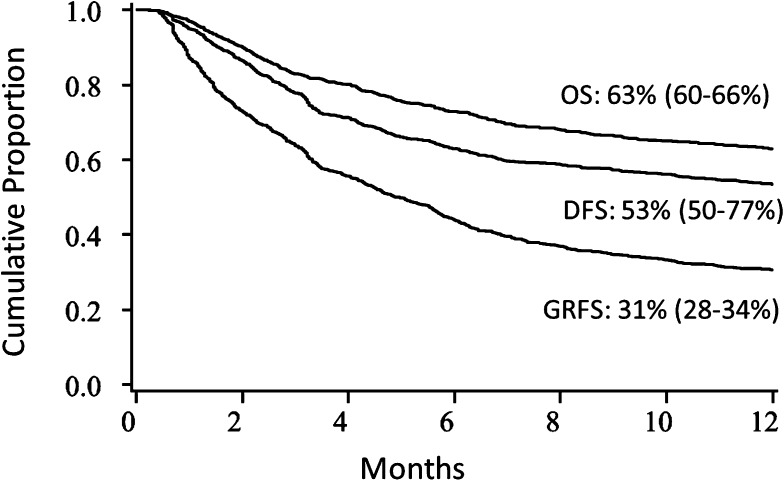
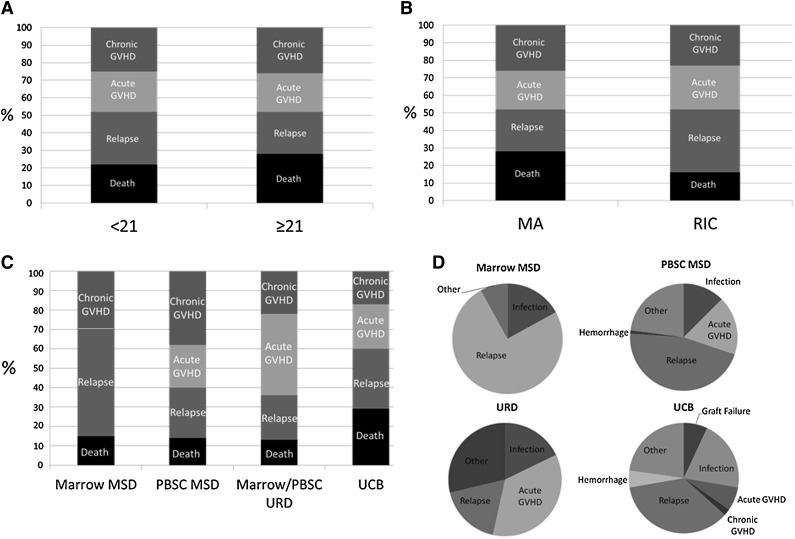
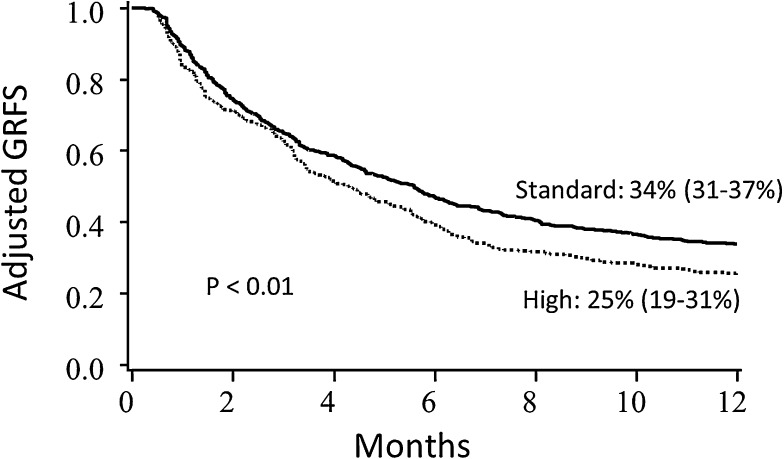
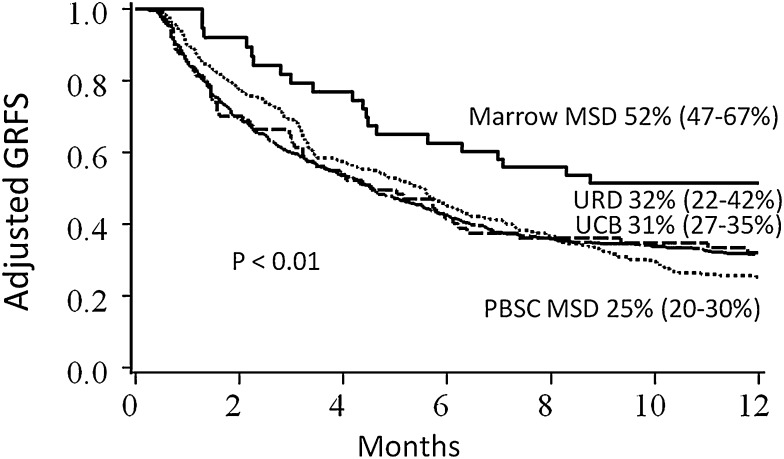
The success of allogeneic hematopoietic cell transplantation (HCT) is typically assessed as individual complications, including graft-versus-host disease (GVHD), relapse, or death, yet no one factor can completely characterize cure without ongoing morbidity. We examined a novel composite end point of GVHD-free/relapse-free survival (GRFS) in which events include grade 3-4 acute GVHD, systemic therapy-requiring chronic GVHD, relapse, or death in the first post-HCT year. In 907 consecutive University of Minnesota allogeneic HCT recipients (2000-2012), 1-year GRFS was 31% (95% confidence interval [CI] 28-34). Regression analyses showed age, disease risk, and donor type significantly influencing GRFS. Adults age 21+ had 2-fold worse GRFS vs children; GRFS did not differ beyond age 21. Adjusted for conditioning intensity, stem cell source, disease risk, age, and transplant year, HLA-matched sibling donor marrow resulted in the best GRFS (51%, 95% CI 46-66), whereas HLA-matched sibling donor peripheral blood stem cells were significantly worse (25%, 95% CI 20-30, P = .01). GRFS after umbilical cord blood transplants and marrow from matched unrelated donors were similar (31%, 95% CI 27-35 and 32%, 95% CI 22-42, respectively). Because GRFS measures freedom from ongoing morbidity and represents ideal HCT recovery, GRFS has value as a novel end point for benchmarking new therapies.
© 2015 by The American Society of Hematology.
Figures
References
-
- Sehn LH, Alyea EP, Weller E, et al. Comparative outcomes of T-cell-depleted and non-T-cell-depleted allogeneic bone marrow transplantation for chronic myelogenous leukemia: impact of donor lymphocyte infusion. J Clin Oncol. 1999;17(2):561–568. - PubMed
-
- Alyea E, Neuberg D, Mauch P, et al. Effect of total body irradiation dose escalation on outcome following T-cell-depleted allogeneic bone marrow transplantation. Biol Blood Marrow Transplant. 2002;8(3):139–144. - PubMed
-
- Sankoh AJ, Li H, D’Agostino RB., Sr Use of composite endpoints in clinical trials. Stat Med. 2014;33(27):4709–4714. - PubMed
-
- Bolanos-Meade J, Koreth J, Reshef R. A multi-center phase II trial randomizing novel approaches for graft-versus-host disease prevention compared to contemporary controls (1203). Available at: https://clinicaltrials.gov/ct2/show/NCT02208037. Accessed January 19, 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
