

Management of thoracolumbar spine trauma: An overview
- PMID: 25593358
- PMCID: PMC4292328
- DOI: 10.4103/0019-5413.143914
Management of thoracolumbar spine trauma: An overview
Abstract
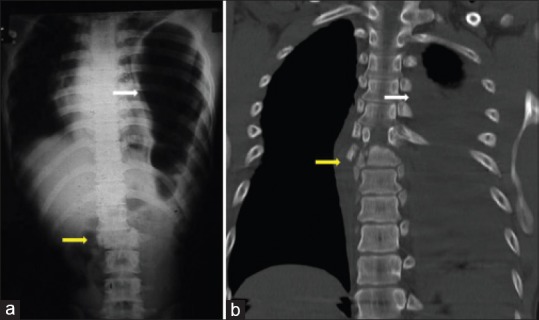
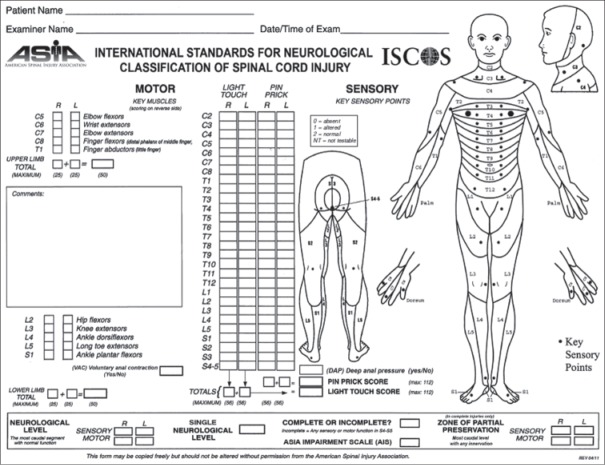
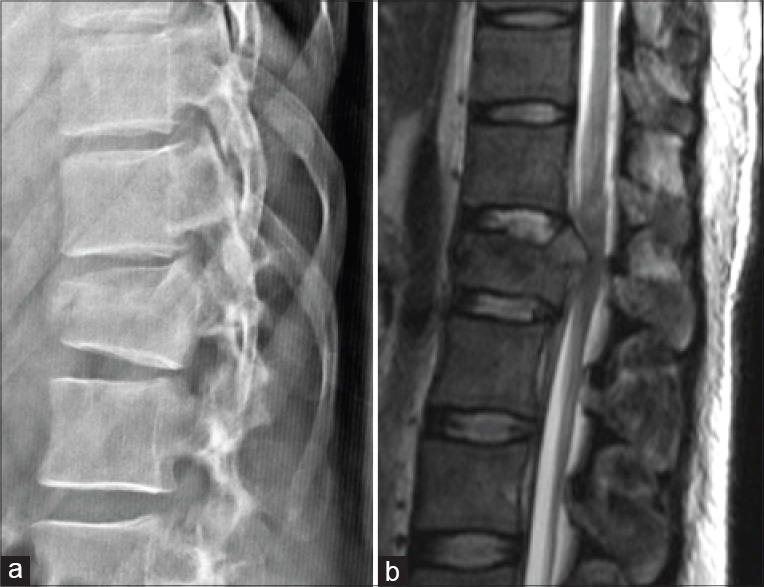
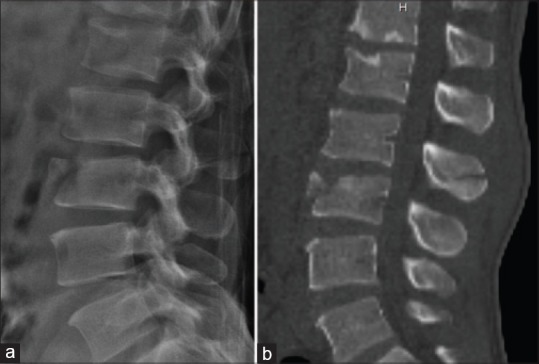
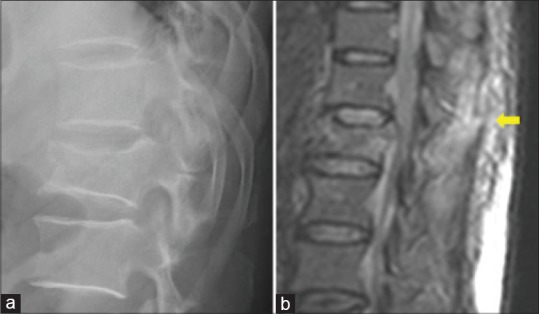
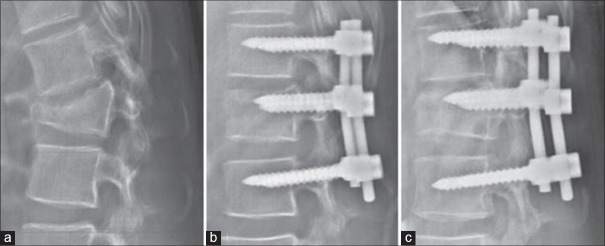
Thoracolumbar spine fractures are common injuries that can result in significant disability, deformity and neurological deficit. Controversies exist regarding the appropriate radiological investigations, the indications for surgical management and the timing, approach and type of surgery. This review provides an overview of the epidemiology, biomechanical principles, radiological and clinical evaluation, classification and management principles. Literature review of all relevant articles published in PubMed covering thoracolumbar spine fractures with or without neurologic deficit was performed. The search terms used were thoracolumbar, thoracic, lumbar, fracture, trauma and management. All relevant articles and abstracts covering thoracolumbar spine fractures with and without neurologic deficit were reviewed. Biomechanically the thoracolumbar spine is predisposed to a higher incidence of spinal injuries. Computed tomography provides adequate bony detail for assessing spinal stability while magnetic resonance imaging shows injuries to soft tissues (posterior ligamentous complex [PLC]) and neurological structures. Different classification systems exist and the most recent is the AO spine knowledge forum classification of thoracolumbar trauma. Treatment includes both nonoperative and operative methods and selected based on the degree of bony injury, neurological involvement, presence of associated injuries and the integrity of the PLC. Significant advances in imaging have helped in the better understanding of thoracolumbar fractures, including information on canal morphology and injury to soft tissue structures. The ideal classification that is simple, comprehensive and guides management is still elusive. Involvement of three columns, progressive neurological deficit, significant kyphosis and canal compromise with neurological deficit are accepted indications for surgical stabilization through anterior, posterior or combined approaches.
Keywords: Spinal injuries; lumbar vertebrae; management; thoracic vertebrae; thoracolumbar trauma; treatment protocols.
Conflict of interest statement
Figures

References
-
- Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014;14:145–64. - PubMed
-
- el-Khoury GY, Whitten CG. Trauma to the upper thoracic spine: Anatomy, biomechanics, and unique imaging features. AJR Am J Roentgenol. 1993;160:95–102. - PubMed
-
- Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine (Phila Pa 1976) 1996;21:492–9. - PubMed
-
- Gertzbein SD. Scoliosis Research Society. Multicenter spine fracture study. Spine (Phila Pa 1976) 1992;17:528–40. - PubMed
-
- Gertzbein SD, Khoury D, Bullington A, St John TA, Larson AI. Thoracic and lumbar fractures associated with skiing and snowboarding injuries according to the AO Comprehensive Classification. Am J Sports Med. 2012;40:1750–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical