

Management of skeletal metastases: An orthopaedic surgeon's guide
- PMID: 25593359
- PMCID: PMC4292329
- DOI: 10.4103/0019-5413.143915
Management of skeletal metastases: An orthopaedic surgeon's guide
Abstract
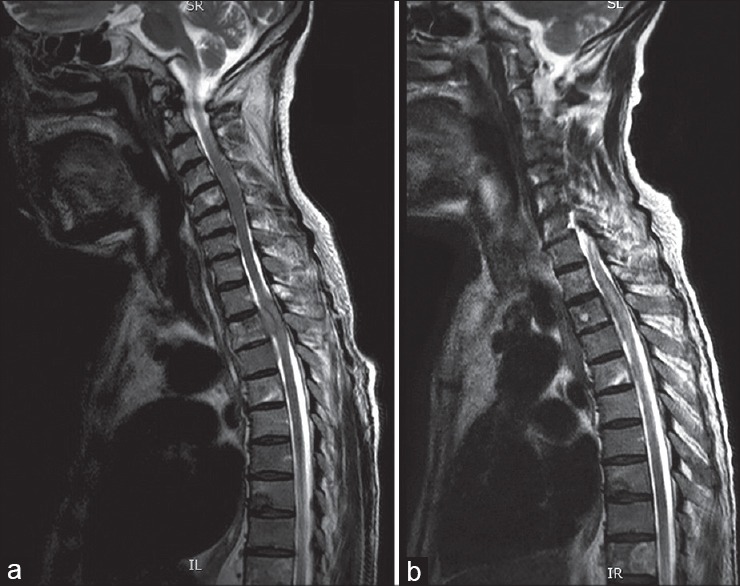
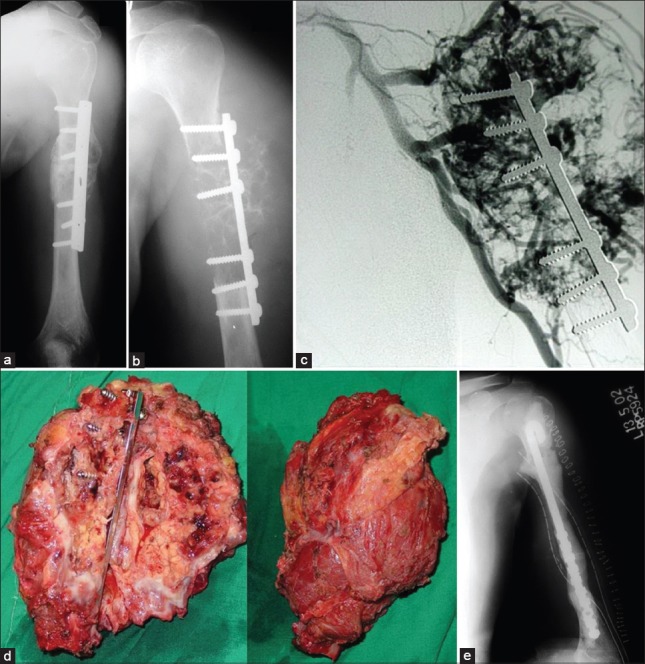
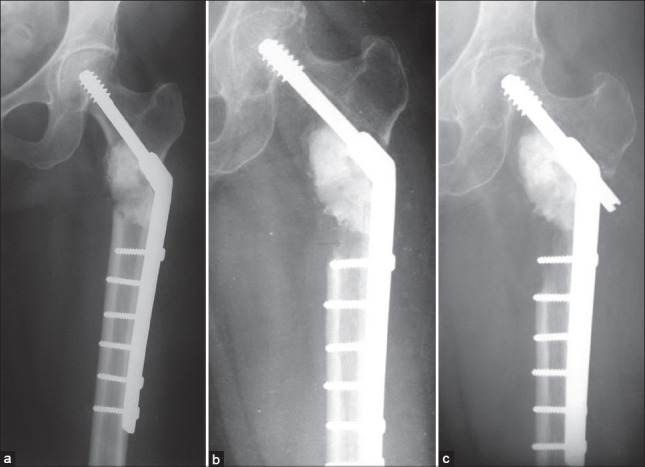
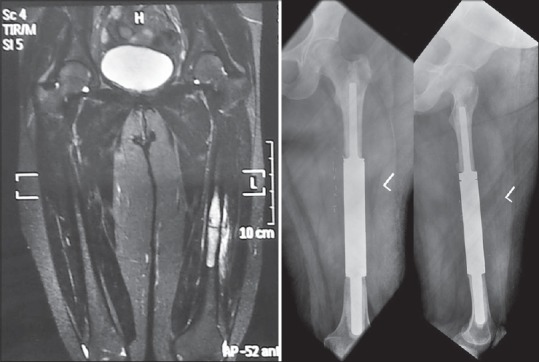
Skeletal metastasis is a common cause of severe morbidity, reduction in quality of life (QOL) and often early mortality. Its prevalence is rising due to a higher rate of diagnosis, better systemic treatment, longer lives with the disease and higher disease burden rate. As people with cancer live longer and with rising sensitivity of body imaging and surveillance, the incidence of pathological fracture, metastatic epidural cord compression is rising and constitutes a challenge for the orthopedic surgeon to maintain their QOL. Metastatic disease is no longer a death sentence condemning patients to "terminal care." In the era of multidisciplinary care and effective systemic targeted and nontargeted therapy, patient expectations of QOL, even during palliative end of care period is high. We lay emphasis on proving the diagnosis of metastasis by biopsy and histopathology and discuss imaging modalities to help estimate fracture risk and map disease extent. This article discusses at length the evidence and decision-making process of various modalities to treat skeletal metastasis. The modalities range from radiation including image-guided, stereotactic and whole body radiation, systemic targeted or hormonal therapy, spinal decompression with or without stabilization, extended curettage with stabilization, resection in select cases with megaprosthetic or biological reconstruction, percutaneous procedures using radio frequency ablation, cementoplasties and discusses the role of emerging modalities like high frequency ultrasound-guided ablation, cryotherapy and whole body radionuclide therapy. The focus lies on the role of multidisciplinary care, which considers complex decisions on patient centric prognosis, comorbidities, cost, feasibility and expectations in order to maximize outcomes on QOL issues.
Keywords: Bone metastases; Metastases; bone cancer; fracture; pathological; pathological fracture; skeletal metastases.
Conflict of interest statement
Figures


Similar articles
-
Current Overview of Treatment for Metastatic Bone Disease.Curr Oncol. 2021 Aug 29;28(5):3347-3372. doi: 10.3390/curroncol28050290. Curr Oncol. 2021. PMID: 34590591 Free PMC article. Review.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
An Overview of Decision Making in the Management of Metastatic Spinal Tumors.Indian J Orthop. 2021 Mar 6;55(4):799-814. doi: 10.1007/s43465-021-00368-8. eCollection 2021 Aug. Indian J Orthop. 2021. PMID: 34194637 Free PMC article. Review.
-
Risk Factors for Pathological Fracture and Metastatic Epidural Spinal Cord Compression in Patients With Spinal Metastases.Orthopedics. 2018 Jan 1;41(1):e38-e45. doi: 10.3928/01477447-20171106-06. Epub 2017 Nov 14. Orthopedics. 2018. PMID: 29136257
-
Conventional Radiotherapy and Stereotactic Radiosurgery in the Management of Metastatic Spine Disease.Technol Cancer Res Treat. 2020 Jan-Dec;19:1533033820945798. doi: 10.1177/1533033820945798. Technol Cancer Res Treat. 2020. PMID: 32757820 Free PMC article. Review.
Cited by
-
Interventional Pain Management for Sacroiliac Tumors in the Oncologic Population: A Case Series and Paradigm Approach.Pain Med. 2017 May 1;18(5):959-968. doi: 10.1093/pm/pnw211. Pain Med. 2017. PMID: 28339540 Free PMC article.
-
Investigation of thermally induced damage to surrounding nerve tissue when using curettage and cementation of long bone tumours, modelled in cadaveric porcine femurs.Arch Orthop Trauma Surg. 2019 Aug;139(8):1033-1038. doi: 10.1007/s00402-019-03129-3. Epub 2019 Feb 4. Arch Orthop Trauma Surg. 2019. PMID: 30715569 Free PMC article.
-
A Patient-Specific Fracture Risk Assessment Tool for Femoral Bone Metastases: Using the Bone Strength (BOS) Score in Clinical Practice.Cancers (Basel). 2022 Nov 29;14(23):5904. doi: 10.3390/cancers14235904. Cancers (Basel). 2022. PMID: 36497388 Free PMC article.
-
Principles of Management of Extremity Skeletal Metastasis.Indian J Palliat Care. 2019 Oct-Dec;25(4):580-586. doi: 10.4103/IJPC.IJPC_90_19. Indian J Palliat Care. 2019. PMID: 31673216 Free PMC article.
-
Effect of Bone Metastasis Cancer Board on Spinal Surgery Outcomes: A Retrospective Study.Medicina (Kaunas). 2023 Nov 28;59(12):2087. doi: 10.3390/medicina59122087. Medicina (Kaunas). 2023. PMID: 38138190 Free PMC article. Review.
References
-
- Rubens RD, Mundy GR. London (UK): Martin Dunitz; 2000. Cancer and the Skeleton.
-
- Rosen LS, Gordon D, Tchekmedyian S, Yanagihara R, Hirsh V, Krzakowski M, et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: A phase iii, double-blind, randomized trial-The zoledronic acid lung cancer and other solid tumors study group. J Clin Oncol. 2003;21:3150–7. - PubMed
-
- Rosen LS, Gordon D, Kaminski M, Howell A, Belch A, Mackey J, et al. Long term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: A randomized, double-blind, multicenter, comparative trial. Cancer. 2003;98:1735–44. - PubMed
-
- Aaron AD. Current concepts review-treatment of metastatic adenocarcinoma of the pelvis and the extremities*. J Bone Joint Surg. 1997;79:917–32. - PubMed
-
- Harrington KD. Orthopaedic management of extremity and pelvic lesions. Clin Orthop Relat Res. 1995:136–47. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials