

Quantitative validation of a computer-aided maxillofacial planning system, focusing on soft tissue deformations
- PMID: 25593866
- PMCID: PMC4293837
- DOI: 10.4103/2231-0746.147112
Quantitative validation of a computer-aided maxillofacial planning system, focusing on soft tissue deformations
Abstract
Aim: The aim of this study was to evaluate the accuracy of 3D soft tissue predictions generated by a computer-aided maxillofacial planning system in patients undergoing orthognathic surgery.
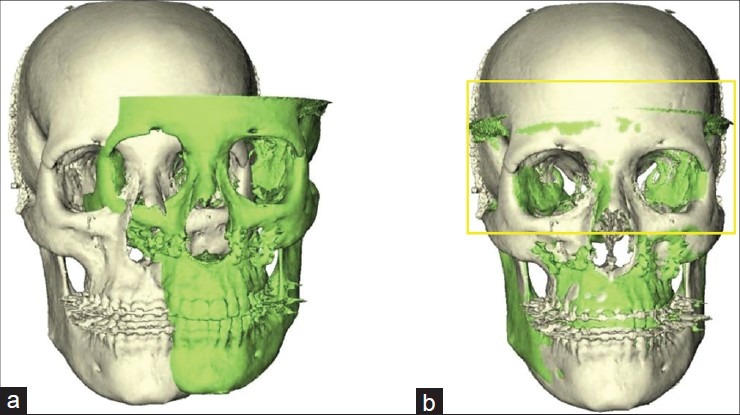
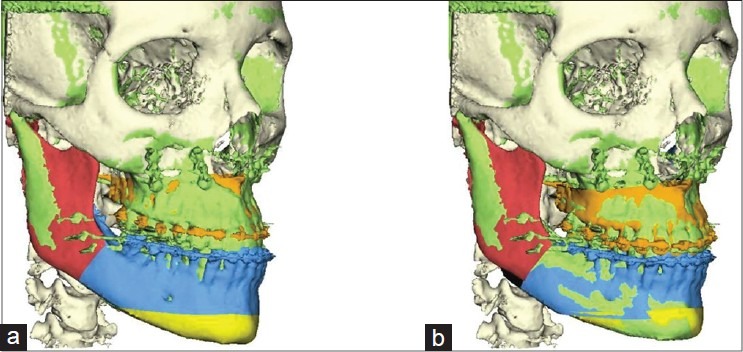
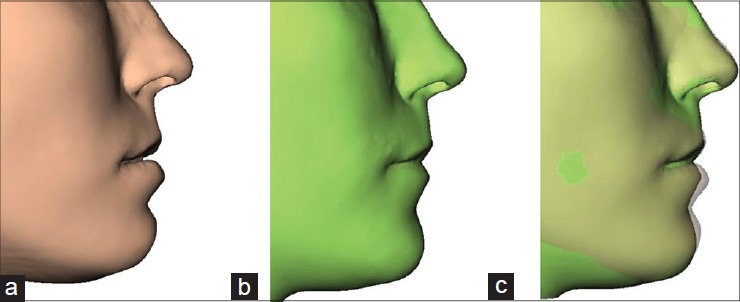
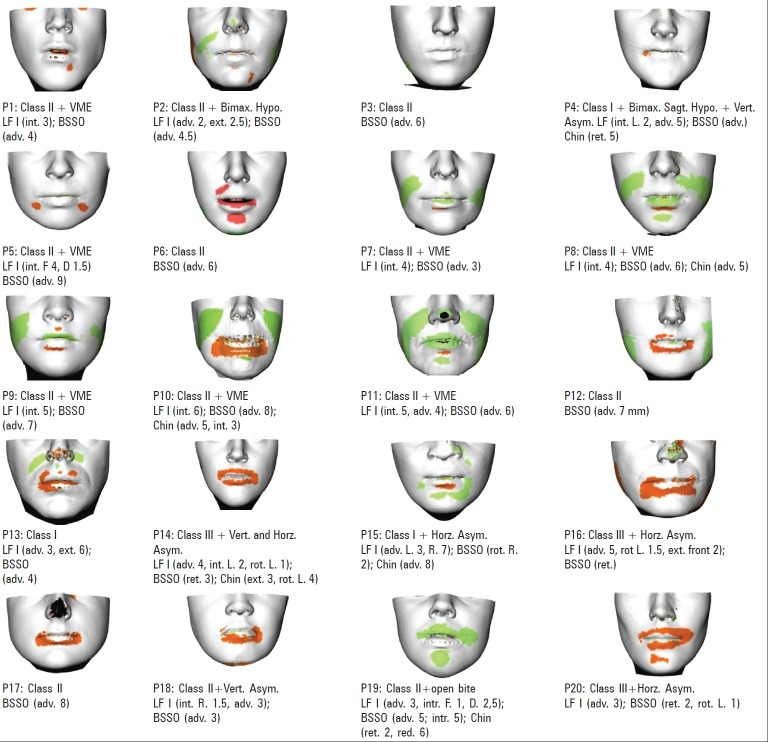
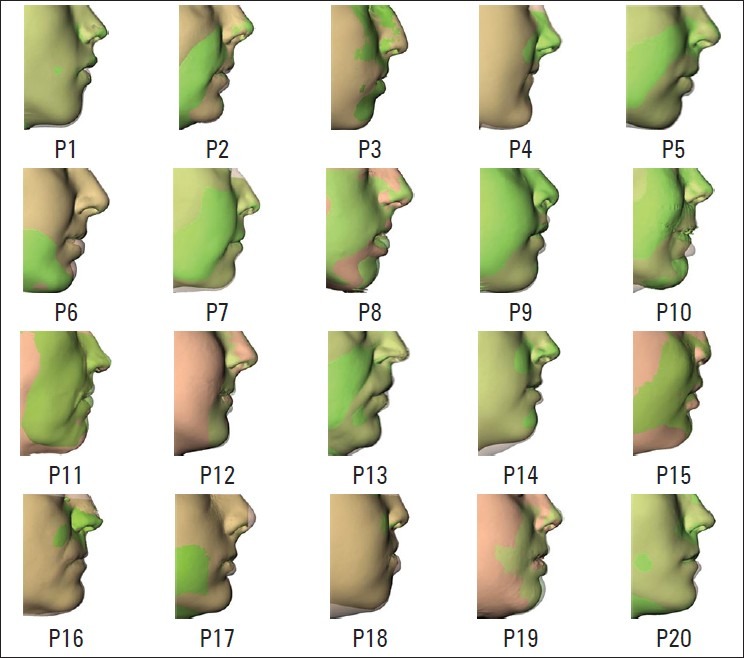
Methods and materials: Twenty patients with dentofacial dysmorphosis were treated with orthognathic surgery after a preoperative orthodontic treatment. Fourteen patients had an Angle Class II malocclusion; three patients had an Angle class III malocclusion, and three patients had an Angle Class I malocclusion. Skeletal asymmetry was observed in six patient. The surgeries were planned using the Maxilim software. Computer assisted surgical planning was transferred to the patient by digitally generated splints. The validation procedures were performed in the following steps: (1) Standardized registration of the pre- and postoperative Cone Beam CT volumes; (2) Automated adjustment of the bone-related planning to the actual operative bony displacement; (3) Simulation of soft tissue changes; (4) Calculation of the soft tissue differences between the predicted and the postoperative results by distance mapping.
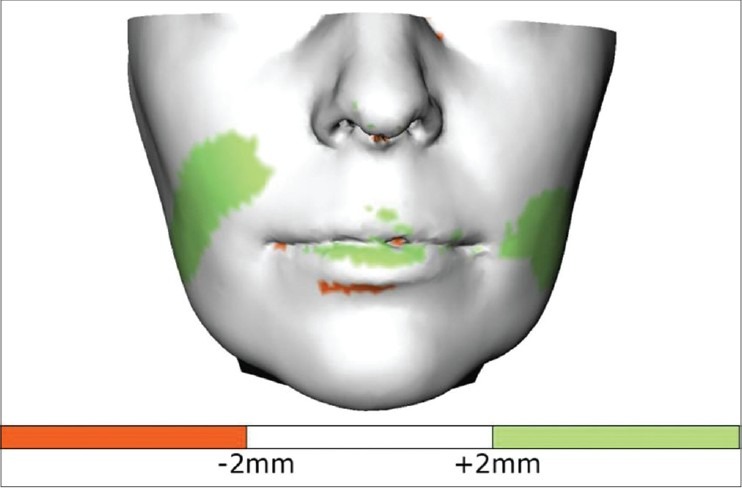
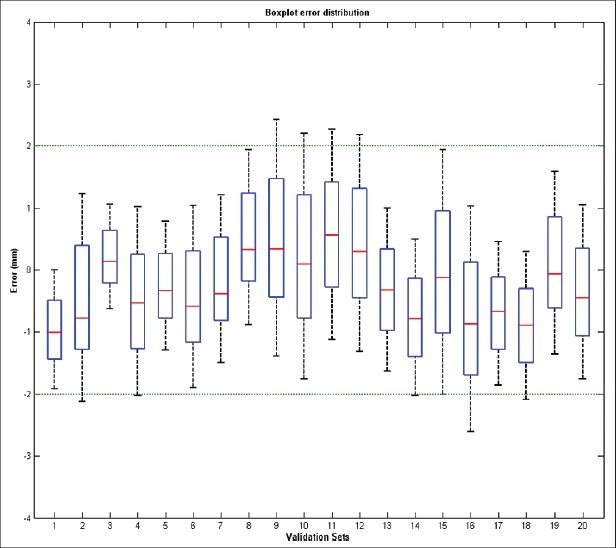
Statistical analysis and results: Eighty four percent of the mapped distances between the predicted and actual postoperative results measured between -2 mm and +2 mm. The mean absolute linear measurements between the predicted and actual postoperative surface was 1.18. Our study shows the overall prediction was dependent on neither the surgical procedures nor the dentofacial deformity type.
Conclusion: Despite some shortcomings in the prediction of the final position of the lower lip and cheek area, this software promises a clinically acceptable soft tissue prediction for orthognathic surgical procedures.
Keywords: 3D planning; orthognathic surgery; soft tissue prediction; virtual surgery.
Conflict of interest statement
Figures

References
-
- Donatsky O, Bjørn-Jørgensen J, Holmqvist-Larsen M, Hillerup S. Computerized cephalometric evaluation of orthognathic surgical precision and stability in relation to maxillary superior repositioning combined with mandibular advancement or setback. J Oral Maxillofac Surg. 1997;55:1071–9. - PubMed
-
- Nadjmi N, Mollemans W, Daelemans A, Van Hemelen G, Schutyser F, Bergé S. Virtual occlusion in planning orthognathic surgical procedures. Int J Oral Maxillofac Surg. 2010;39:457–62. - PubMed
-
- Maes F, Collignon A, Vandermeulen D, Marchal G, Suetens P. Multimodality image registration by maximization of mutual information. IEEE Trans Med Imaging. 1997;16:187–98. - PubMed
-
- Swennen GR, Mollemans W, De Clercq C, Abeloos J, Lamoral P, Lippens F, et al. A cone-beam computed tomography triple scan procedure to obtain a three-dimensional augmented virtual skull model appropriate for orthognathic surgery planning. J Craniofac Surg. 2009;20:297–307. - PubMed
-
- Gateno J, Xia J, Teichgraeber JF, Rosen A, Hultgren B, Vadnais T. The precision of computer-generated surgical splints. J Oral Maxillofac Surg. 2003;61:814–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources