

Integrating funds for health and social care: an evidence review
- PMID: 25595287
- PMCID: PMC4469543
- DOI: 10.1177/1355819614566832
Integrating funds for health and social care: an evidence review
Abstract
Objectives: Integrated funds for health and social care are one possible way of improving care for people with complex care requirements. If integrated funds facilitate coordinated care, this could support improvements in patient experience, and health and social care outcomes, reduce avoidable hospital admissions and delayed discharges, and so reduce costs. In this article, we examine whether this potential has been realized in practice.
Methods: We propose a framework based on agency theory for understanding the role that integrated funding can play in promoting coordinated care, and review the evidence to see whether the expected effects are realized in practice. We searched eight electronic databases and relevant websites, and checked reference lists of reviews and empirical studies. We extracted data on the types of funding integration used by schemes, their benefits and costs (including unintended effects), and the barriers to implementation. We interpreted our findings with reference to our framework.
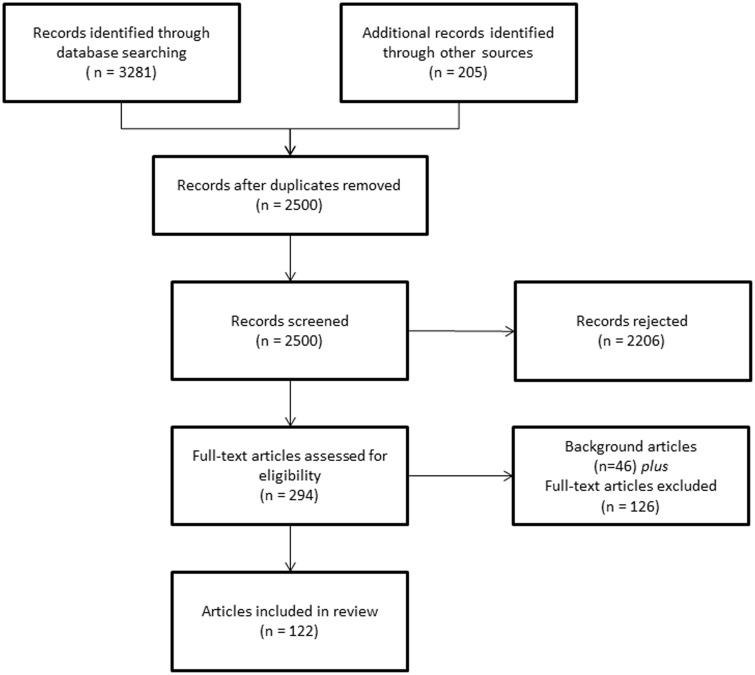
Results: The review included 38 schemes from eight countries. Most of the randomized evidence came from Australia, with nonrandomized comparative evidence available from Australia, Canada, England, Sweden and the US. None of the comparative evidence isolated the effect of integrated funding; instead, studies assessed the effects of 'integrated financing plus integrated care' (i.e. 'integration') relative to usual care. Most schemes (24/38) assessed health outcomes, of which over half found no significant impact on health. The impact of integration on secondary care costs or use was assessed in 34 schemes. In 11 schemes, integration had no significant effect on secondary care costs or utilisation. Only three schemes reported significantly lower secondary care use compared with usual care. In the remaining 19 schemes, the evidence was mixed or unclear. Some schemes achieved short-term reductions in delayed discharges, but there was anecdotal evidence of unintended consequences such as premature hospital discharge and heightened risk of readmission. No scheme achieved a sustained reduction in hospital use. The primary barrier was the difficulty of implementing financial integration, despite the existence of statutory and regulatory support. Even where funds were successfully pooled, budget holders' control over access to services remained limited. Barriers in the form of differences in performance frameworks, priorities and governance were prominent amongst the UK schemes, whereas difficulties in linking different information systems were more widespread. Despite these barriers, many schemes - including those that failed to improve health or reduce costs - reported that access to care had improved. Some of these schemes revealed substantial levels of unmet need and so total costs increased.
Conclusions: It is often assumed in policy that integrating funding will promote integrated care, and lead to better health outcomes and lower costs. Both our agency theory-based framework and the evidence indicate that the link is likely to be weak. Integrated care may uncover unmet need. Resolving this can benefit both individuals and society, but total care costs are likely to rise. Provided that integration delivers improvements in quality of life, even with additional costs, it may, nonetheless, offer value for money.
Keywords: integrated care; joint commissioning; payment systems; pooled budgets; systematic review.
© The Author(s) 2015.
Figures
References
-
- Dickinson H, Glasby J. ‘Why partnership working doesn’t work’: pitfalls, problems and possibilities in English health and social care. Publ Manag Rev 2010; 12: 811–828.
-
- Lynch M, Estes CL, Hernandez M. Chronic care initiatives for the elderly: can they bridge the gerontology–medicine gap? J Appl Gerontol 2005; 24: 108–124.
-
- Williams I, Dickinson H, Robinson S. Joined-up rationing?: an analysis of priority setting in health and social care commissioning. J Integr Care 2011; 19: 3–11.
-
- Department of Health, National Collaboration for Integrated Care and Support. Integrated care: our shared commitment. A framework that outlines ways to improve health and social care integration. London: Department of Health, 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
