

Impact of age and medical comorbidity on adjuvant treatment outcomes for stage III colon cancer: a pooled analysis of individual patient data from four randomized, controlled trials
- PMID: 25595934
- PMCID: PMC4374386
- DOI: 10.1093/annonc/mdv003
Impact of age and medical comorbidity on adjuvant treatment outcomes for stage III colon cancer: a pooled analysis of individual patient data from four randomized, controlled trials
Abstract
Background: Adjuvant oxaliplatin plus capecitabine or leucovorin/5-fluorouracil (LV/5-FU) (XELOX/FOLFOX) is the standard of care for stage III colon cancer (CC); however, there is disagreement regarding oxaliplatin benefit in patients aged >70. In most analyses, the impact of medical comorbidity (MC) has not been assessed. Efficacy and safety of adjuvant XELOX/FOLFOX versus LV/5-FU were compared with respect to age and MC using pooled data from four randomized, controlled trials, selected for access to patient-level MC data and including commonly endorsed and utilized regimens.
Patients and methods: Individual data from patients with stage III CC in NSABP C-08, XELOXA, X-ACT, and AVANT were pooled, excluding bevacizumab-treated patients. Patients were grouped by treatment, MC (low versus high), or age (<70 versus ≥70), and compared for disease-free survival (DFS), overall survival (OS), and adverse events (AEs). Multivariable Cox proportional hazards regression controlled for gender, T stage, and N stage.
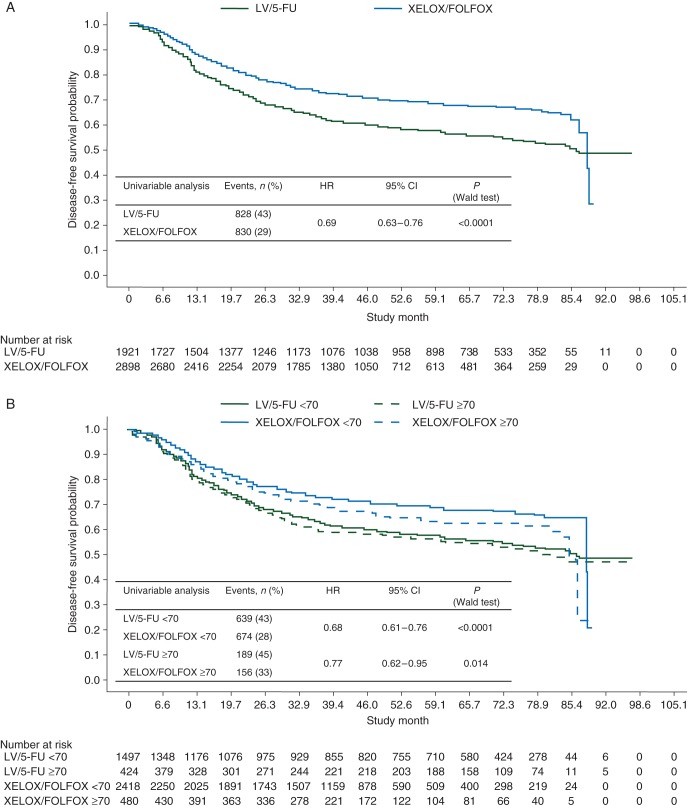
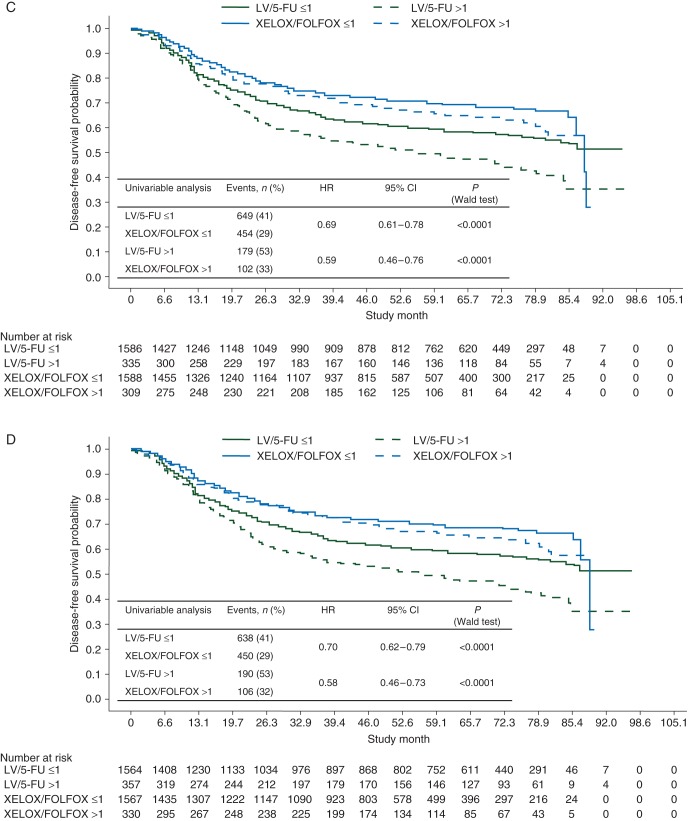
Results: DFS benefits were shown for XELOX/FOLFOX versus LV/5-FU regardless of age or MC, although benefits were modestly attenuated for patients aged ≥70. Hazard ratios were 0.68 (P < 0.0001) and 0.77 (P < 0.014) for <70 and ≥70 age groups; 0.69 (P < 0.0001) and 0.59 (P < 0.0001) for Charlson Comorbidity Index ≤1 and >1 groups; and 0.70 (P < 0.0001) and 0.58 (P < 0.0001) for National Cancer Institute Combined Index ≤1 and >1 groups. OS was also significantly improved in all groups. Grade 3/4 serious AE rates were comparable across cohorts and MC scores and higher in patients aged ≥70. Oxaliplatin-relevant grade 3/4 AEs, including neuropathy, were comparable across ages and MC scores.
Conclusions: Results further support consideration of XELOX or FOLFOX as standard treatment options for the adjuvant management of stage III CC in all age groups and in patients with comorbidities, consistent with those who were eligible for these clinical trials.
Keywords: adjuvant chemotherapy; age groups; capecitabine; colon cancer; comorbidity; oxaliplatin.
© The Author 2015. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- André T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004; 350: 2343–2351. - PubMed
-
- André T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 2009; 27: 3109–3116. - PubMed
-
- Haller DG, Tabernero J, Maroun J, et al. Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer. J Clin Oncol 2011; 29: 1465–1471. - PubMed
-
- Schmoll H-J, Tabernero J, Maroun JA, et al. Capecitabine plus oxaliplatin (XELOX) versus bolus 5-fluorouracil/leucovorin (5-FU/LV) as adjuvant therapy for stage III colon cancer: survival follow-up of study NO16968 (XELOXA). J Clin Oncol 2012; 30: Abstr 338.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
