

Recent advances in image-guided targeted prostate biopsy
- PMID: 25596716
- PMCID: PMC6666428
- DOI: 10.1007/s00261-015-0353-8
Recent advances in image-guided targeted prostate biopsy
Abstract
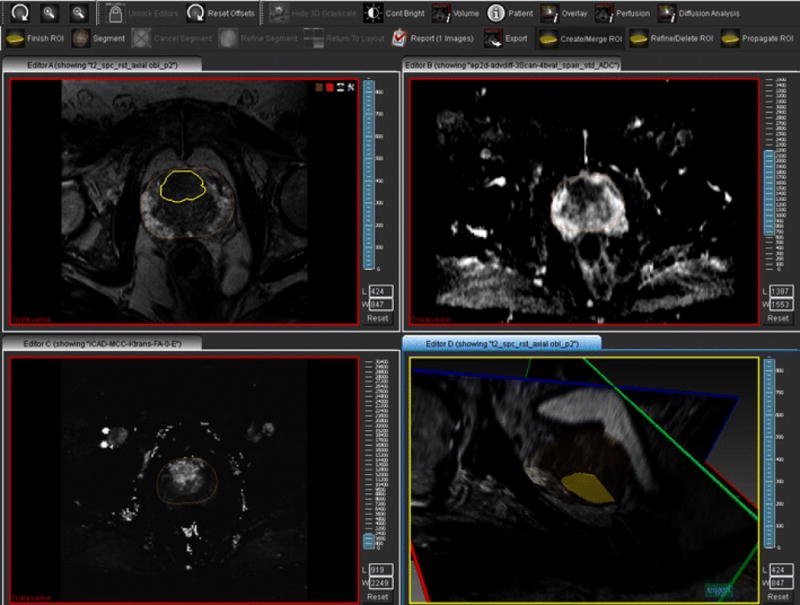
Prostate cancer is a common malignancy in the United States that results in over 30,000 deaths per year. The current state of prostate cancer diagnosis, based on PSA screening and sextant biopsy, has been criticized for both overdiagnosis of low-grade tumors and underdiagnosis of clinically significant prostate cancers (Gleason score ≥7). Recently, image guidance has been added to perform targeted biopsies of lesions detected on multi-parametric magnetic resonance imaging (mpMRI) scans. These methods have improved the ability to detect clinically significant cancer, while reducing the diagnosis of low-grade tumors. Several approaches have been explored to improve the accuracy of image-guided targeted prostate biopsy, including in-bore MRI-guided, cognitive fusion, and MRI/transrectal ultrasound fusion-guided biopsy. This review will examine recent advances in these image-guided targeted prostate biopsy techniques.
Figures




References
-
- What are the key statistics about prostate cancer? 2013:1. www.cancer.org.
-
- Lazzeri M, Abrate A, Lughezzani G, et al. Relationship of chronic histologic prostatic inflammation in biopsy specimens with serum isoform [−2]proPSA (p2PSA), %p2PSA, and prostate health index in men with a total prostate-specific antigen of 4–10 ng/ml and normal digital rectal examination. Urology. 2014;83:606–12. doi: 10.1016/j.urology.2013.10.016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
