

Upper extremity 3-dimensional reachable workspace analysis in dystrophinopathy using Kinect
- PMID: 25597487
- PMCID: PMC4506893
- DOI: 10.1002/mus.24567
Upper extremity 3-dimensional reachable workspace analysis in dystrophinopathy using Kinect
Abstract
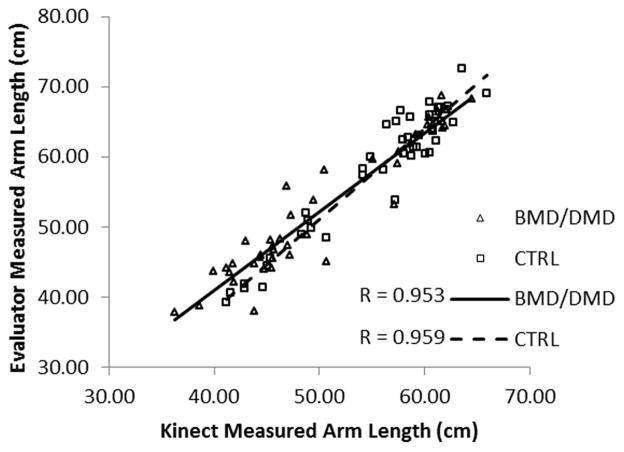
Introduction: An innovative upper extremity 3-dimensional (3D) reachable workspace outcome measure acquired using the Kinect sensor is applied toward Duchenne/Becker muscular dystrophy (DMD/BMD). The validity, sensitivity, and clinical meaningfulness of this novel outcome measure are examined.
Methods: Upper extremity function assessment (Brooke scale and NeuroQOL questionnaire) and Kinect-based reachable workspace analyses were conducted in 43 individuals with dystrophinopathy (30 DMD and 13 BMD, aged 7-60 years) and 46 controls (aged 6-68 years).
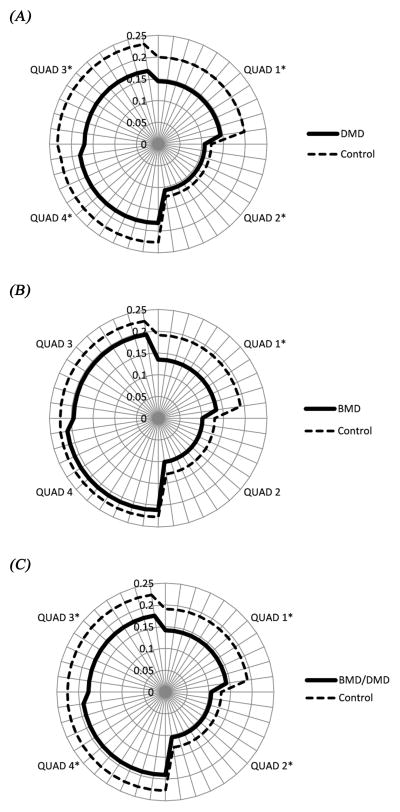
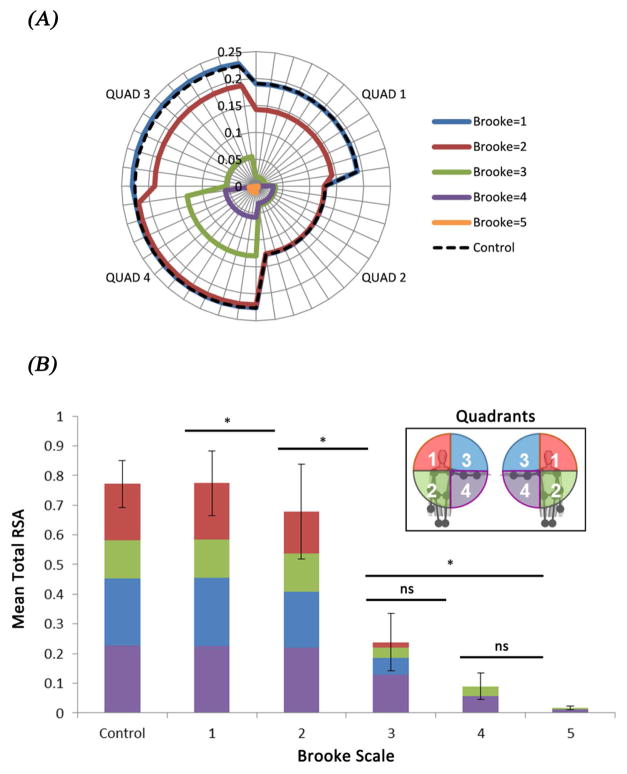
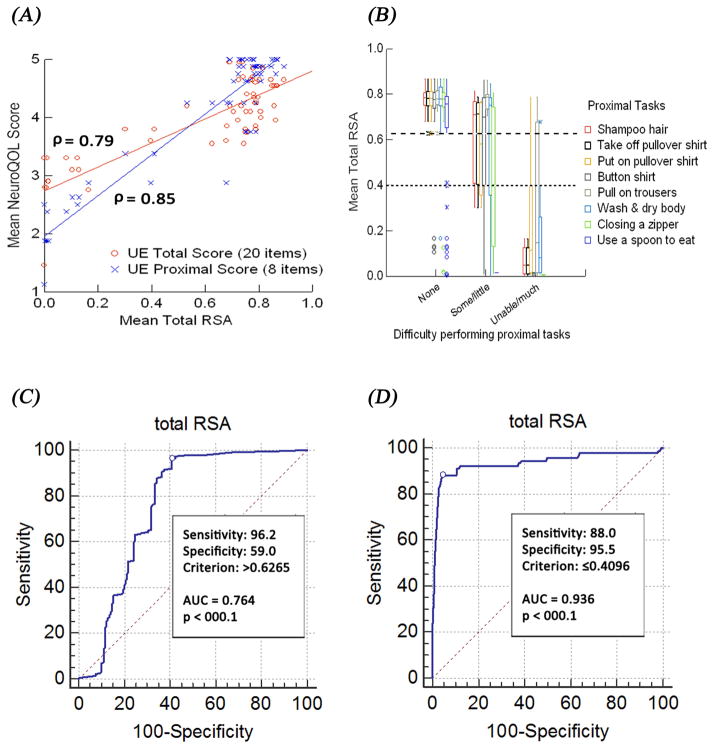
Results: The reachable workspace measure reliably captured a wide range of upper extremity impairments encountered in both pediatric and adult, as well as ambulatory and non-ambulatory individuals with dystrophinopathy. Reduced reachable workspaces were noted for the dystrophinopathy cohort compared with controls, and they correlated with Brooke grades. In addition, progressive reduction in reachable workspace correlated directly with worsening ability to perform activities of daily living, as self-reported on the NeuroQOL.
Conclusion: This study demonstrates the utility and potential of the novel sensor-acquired reachable workspace outcome measure in dystrophinopathy.
Keywords: Becker; Duchenne; Kinect; reachable workspace; upper extremity.
© 2015 Wiley Periodicals, Inc.
Figures



References
-
- Emery AE. Duchenne Muscular Dystrophy – Meryon’s disease. Neuromuscul Disord. 1993 Jul;3(4):263–6. - PubMed
-
- Prevalence of Duchenne/Becker muscular dystrophy among males aged 5–24 years-four states, 2007. MMWR Morb Mortal Wkly Rep. 2009;58:1119–1122. - PubMed
-
- Hoffman EP, Brown RH, Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell. 1987 Dec 24;51(6):919–28. - PubMed
-
- Aartsma-Rus A, Van Deutekom JC, Fokkema IF, Van Ommen GJ, Den Dunnen JT. Entries in the Leiden Duchenne muscular dystrophy mutation database: an overview of mutation types and paradoxical cases that confirm the reading-frame rule. Muscle Nerve. 2006 Aug;34(2):135–44. Review. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
