

Retrospective study of the effectiveness of Intra-Aortic Balloon Occlusion (IABO) for traumatic haemorrhagic shock
- PMID: 25598838
- PMCID: PMC4297416
- DOI: 10.1186/1749-7922-10-1
Retrospective study of the effectiveness of Intra-Aortic Balloon Occlusion (IABO) for traumatic haemorrhagic shock
Abstract
Introduction: Intra-aortic balloon occlusion (IABO) is useful for proximal vascular control, by clamping the descending aorta, in traumatic haemorrhagic shock. However, there are limited clinical studies regarding its effectiveness. This study aimed at investigating the effectiveness of IABO for traumatic haemorrhagic shock.
Methods: This retrospective, observational study included trauma patients who underwent IABO at the Emergency and Critical Care Center of Nippon Medical School Tama-Nagayama Hospital between January 2009 and March 2013. 14 patients were included to this study who were in shock on arrival (systolic blood pressure [SBP] <90 mmHg or shock index ≥1), underwent IABO for resuscitation and temporary haemostasis, and subsequently underwent haemostatic intervention (operation or transcatheter arterial embolization). Patient characteristics, physiological status, SBP, heart rate (HR), initial fluid and blood transfusion, time course, and total occlusion time were compared before and after IABO as well as between the survived (n = 5) and non-survived (n = 9) groups.
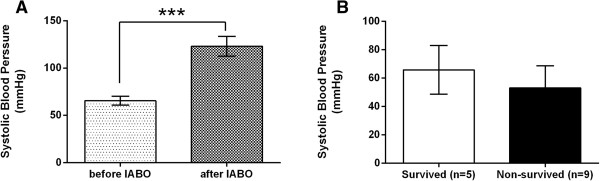
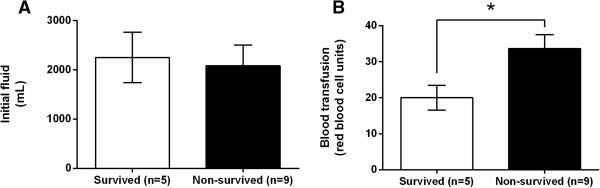
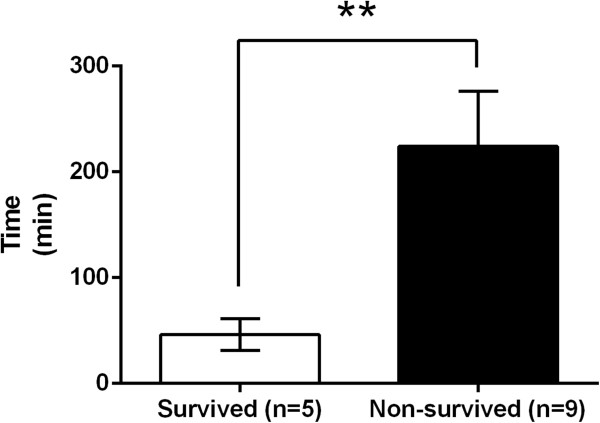
Results: The majority of patients experienced blunt injuries, with an average injury severity score of 29.5. The liver, pelvis, spleen, and mesenterium represented the majority of injured organs. SBP, but not HR, was significantly higher after IABO than before IABO (123.1 vs. 65.5 mmHg, P = 0.0001). The revised trauma score and probability of survival were significantly different between the survived and non-survived groups (both, P = 0.04). The survived group required significantly less blood transfusion volume than the non-survived group (20 vs. 33.7 red blood cell units, P = 0.04). In addition, the survived group required a significantly shorter total occlusion time than the non-survived group (46.2 vs. 224.1 min, P = 0.002).
Conclusions: IABO was used for relatively severe trauma patients. SBP was significantly higher after IABO, but was not related to survival. However, blood transfusion volume and total occlusion time were related to survival; therefore, it is important to reduce or shorten these parameters, i.e., immediate definitive haemostasis. IABO is effective for traumatic haemorrhagic shock; however, it is also important to consider these points and potential complications.
Keywords: Haemorrhagic shock; Intra-aortic balloon occlusion (IABO); Proximal vascular control; Trauma.
Figures

References
-
- Edwards WS, Salter PP, Jr, Carnaggio VA. Intraluminal aortic occlusion as a possible mechanism for controlling massive intra-abdominal hemorrhage. Surg Forum. 1953;4:496–9. - PubMed
-
- Martinelli T, Thony F, Declety P, Sengel C, Broux C, Tonetti J, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma. 2010;68(4):942–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
