

Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer
- PMID: 25599322
- PMCID: PMC4349683
- DOI: 10.1097/SLA.0000000000000867
Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer
Abstract
Purpose: On the basis of the ACCORD trial, FOLFIRINOX is effective in metastatic pancreatic adenocarcinoma (PDAC), making it a rational choice for locally advanced PDAC (LA). Aims of this study are to evaluate the accuracy of imaging in determining the resectability of PDAC and to determine the surgical and clinicopathologic outcomes of pancreatic resections after neoadjuvant FOLFIRINOX therapy.
Patients and methods: Clinicopathologic data were retrospectively collected for surgical PDAC patients receiving neoadjuvant FOLFIRINOX or no neoadjuvant therapy between April 2011 and February 2014. Americas Hepato-Pancreato-Biliary Association/Society of Surgical Oncology/Society for Surgery of the Alimentary Tract consensus guidelines defined LA and borderline. Imaging was reviewed by a blinded senior pancreatic surgeon.
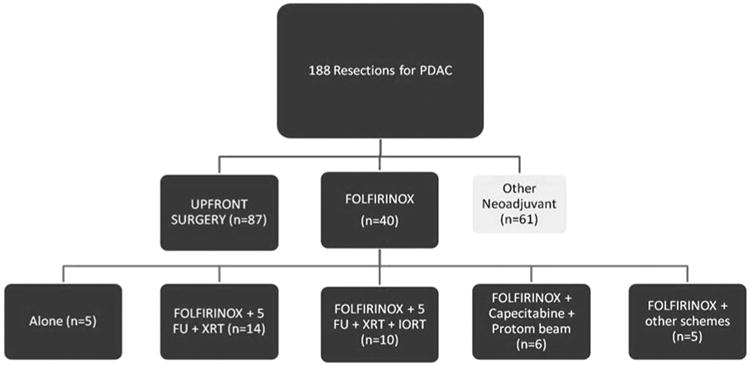
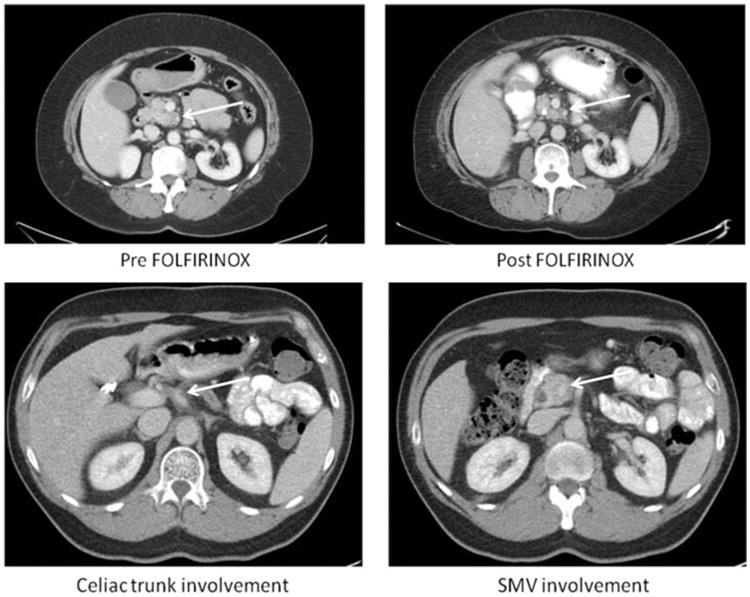
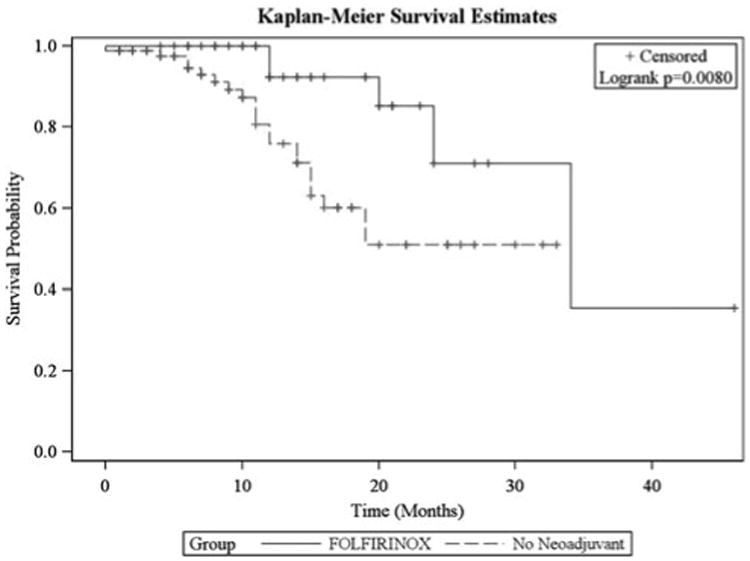
Results: Of 188 patients undergoing resection for PDAC, 40 LA/borderline received FOLFIRINOX and 87 received no neoadjuvant therapy. FOLFIRINOX resulted in a significant decrease in tumor size, yet 19 patients were still classified as LA and 9 as borderline. Despite post-FOLFIRINOX imaging suggesting continued unresectability, 92% had an R0 resection. When compared with no neoadjuvant therapy, FOLFIRINOX resulted in significantly longer operative times (393 vs 300 minutes) and blood loss (600 vs 400 mL), but significantly lower operative morbidity (36% vs 63%) and no postoperative pancreatic fistulas. Length of stay (6 vs 7 days), readmissions (20% vs 30%), and mortality were equivalent (1% vs 0%). On final pathology, the FOLFIRINOX group had a significant decrease in lymph node positivity (35% vs 79%) and perineural invasion (72% vs 95%). Median follow-up was 11 months with a significant increase in overall survival with FOLFIRINOX.
Conclusions: After neoadjuvant FOLFIRINOX imaging no longer predicts unresectability. Traditional pathologic predictors of survival are improved, and morbidity is decreased in comparison to patients with clearly resectable cancers at the time of presentation.
Conflict of interest statement
Disclosure: The authors declare no conflicts of interest.
Figures
Comment in
-
Neoadjuvant therapy for localized pancreatic cancer: support is growing?Ann Surg. 2015 Jan;261(1):18-20. doi: 10.1097/SLA.0000000000000996. Ann Surg. 2015. PMID: 25599323 No abstract available.
-
[After neoadjuvant therapy of pancreatic cancer the classical radiological criteria for resectability are no longer applicable].Chirurg. 2015 Feb;86(2):183. doi: 10.1007/s00104-015-2987-z. Chirurg. 2015. PMID: 25673227 German. No abstract available.
-
"Radiological and Surgical Implications of Neoadjuvant Treatment With FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer.".Ann Surg. 2017 Jun;265(6):E73. doi: 10.1097/SLA.0000000000001322. Ann Surg. 2017. PMID: 28486290 No abstract available.
References
-
- Hidalgo M. Pancreatic cancer. New Engl J Med. 2010;362:1605–1617. - PubMed
-
- Ferrone CR, Brennan MF, Gonen M, et al. Pancreatic adenocarcinoma: the actual 5-year survivors. J Gastrointest Surg. 2008;12:701–706. - PubMed
-
- Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg. 2006;10:1199–1210. discussion 1210–1211. - PubMed
-
- Ko AH, Quivey JM, Venook AP, et al. A phase II study of fixed-dose rate gemcitabine plus low-dose cisplatin followed by consolidative chemoradiation for locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2007;68:809–816. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
