

Fluid management with a simplified conservative protocol for the acute respiratory distress syndrome*
- PMID: 25599463
- PMCID: PMC4675623
- DOI: 10.1097/CCM.0000000000000715
Fluid management with a simplified conservative protocol for the acute respiratory distress syndrome*
Abstract
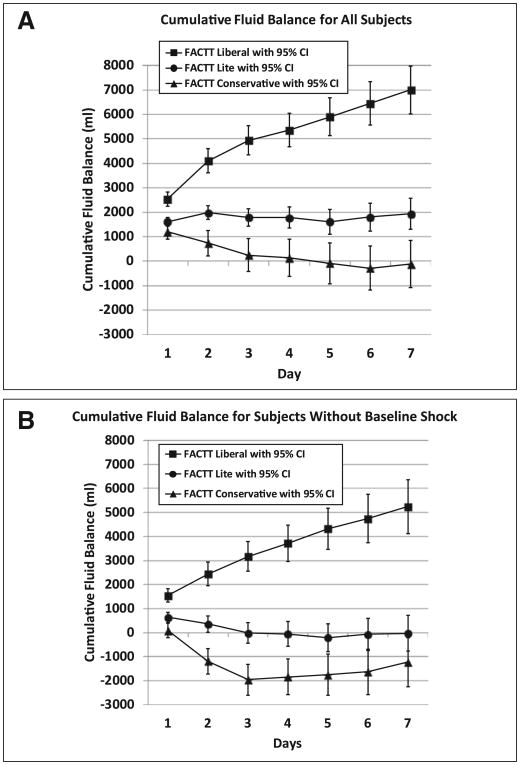
Objectives: In the Fluid and Catheter Treatment Trial (FACTT) of the National Institutes of Health Acute Respiratory Distress Syndrome Network, a conservative fluid protocol (FACTT Conservative) resulted in a lower cumulative fluid balance and better outcomes than a liberal fluid protocol (FACTT Liberal). Subsequent Acute Respiratory Distress Syndrome Network studies used a simplified conservative fluid protocol (FACTT Lite). The objective of this study was to compare the performance of FACTT Lite, FACTT Conservative, and FACTT Liberal protocols.
Design: Retrospective comparison of FACTT Lite, FACTT Conservative, and FACTT Liberal. Primary outcome was cumulative fluid balance over 7 days. Secondary outcomes were 60-day adjusted mortality and ventilator-free days through day 28. Safety outcomes were prevalence of acute kidney injury and new shock.
Setting: ICUs of Acute Respiratory Distress Syndrome Network participating hospitals.
Patients: Five hundred three subjects managed with FACTT Conservative, 497 subjects managed with FACTT Liberal, and 1,124 subjects managed with FACTT Lite.
Interventions: Fluid management by protocol.
Measurements and main results: Cumulative fluid balance was 1,918 ± 323 mL in FACTT Lite, -136 ± 491 mL in FACTT Conservative, and 6,992 ± 502 mL in FACTT Liberal (p < 0.001). Mortality was not different between groups (24% in FACTT Lite, 25% in FACTT Conservative and Liberal, p = 0.84). Ventilator-free days in FACTT Lite (14.9 ± 0.3) were equivalent to FACTT Conservative (14.6 ± 0.5) (p = 0.61) and greater than in FACTT Liberal (12.1 ± 0.5, p < 0.001 vs Lite). Acute kidney injury prevalence was 58% in FACTT Lite and 57% in FACTT Conservative (p = 0.72). Prevalence of new shock in FACTT Lite (9%) was lower than in FACTT Conservative (13%) (p = 0.007 vs Lite) and similar to FACTT Liberal (11%) (p = 0.18 vs Lite).
Conclusions: FACTT Lite had a greater cumulative fluid balance than FACTT Conservative but had equivalent clinical and safety outcomes. FACTT Lite is an alternative to FACTT Conservative for fluid management in Acute Respiratory Distress Syndrome.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Fluid therapy during acute respiratory distress syndrome: less is more, simplified*.Crit Care Med. 2015 Feb;43(2):477-8. doi: 10.1097/CCM.0000000000000794. Crit Care Med. 2015. PMID: 25599472 No abstract available.
-
Fluid Protocol for Acute Respiratory Distress Syndrome, Catheter Thrombolysis for Intermediate Risk Pulmonary Embolism, and Steroids for Community-acquired Pneumonia.Am J Respir Crit Care Med. 2015 Jun 1;191(11):1331-3. doi: 10.1164/rccm.201502-0340RR. Am J Respir Crit Care Med. 2015. PMID: 26029838 No abstract available.
References
-
- The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354:2564–2575. - PubMed
