

Return on investment in electronic health records in primary care practices: a mixed-methods study
- PMID: 25600508
- PMCID: PMC4288109
- DOI: 10.2196/medinform.3631
Return on investment in electronic health records in primary care practices: a mixed-methods study
Abstract
Background: The use of electronic health records (EHR) in clinical settings is considered pivotal to a patient-centered health care delivery system. However, uncertainty in cost recovery from EHR investments remains a significant concern in primary care practices.
Objective: Guided by the question of "When implemented in primary care practices, what will be the return on investment (ROI) from an EHR implementation?", the objectives of this study are two-fold: (1) to assess ROI from EHR in primary care practices and (2) to identify principal factors affecting the realization of positive ROI from EHR. We used a break-even point, that is, the time required to achieve cost recovery from an EHR investment, as an ROI indicator of an EHR investment.
Methods: Given the complexity exhibited by most EHR implementation projects, this study adopted a retrospective mixed-method research approach, particularly a multiphase study design approach. For this study, data were collected from community-based primary care clinics using EHR systems.
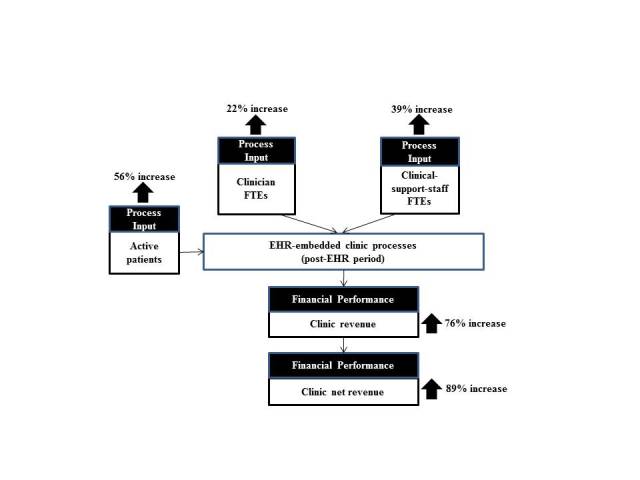
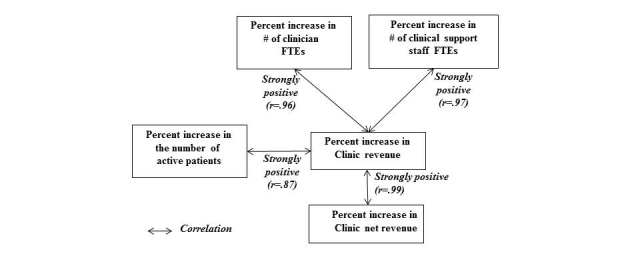
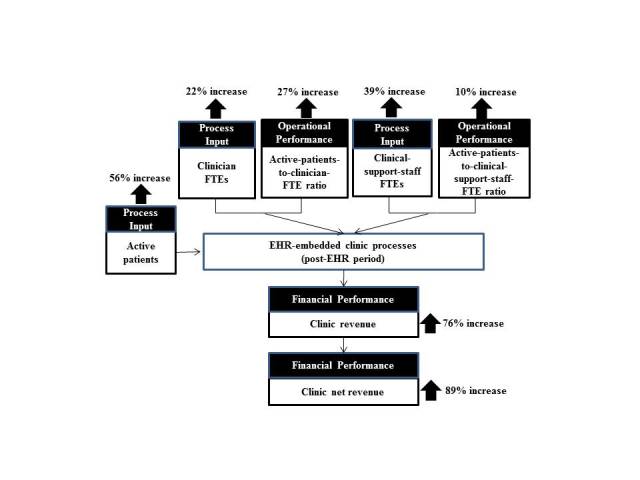
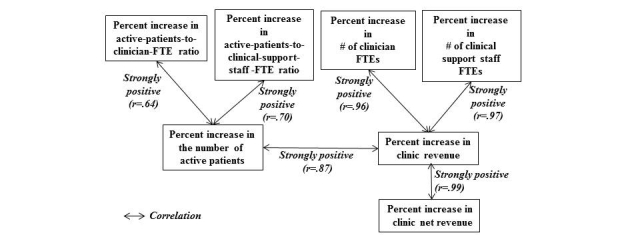
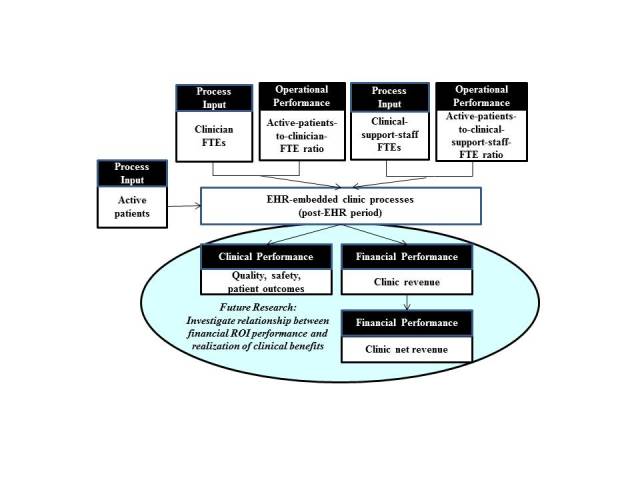
Results: We collected data from 17 primary care clinics using EHR systems. Our data show that the sampled primary care clinics recovered their EHR investments within an average period of 10 months (95% CI 6.2-17.4 months), seeing more patients with an average increase of 27% in the active-patients-to-clinician-FTE (full time equivalent) ratio and an average increase of 10% in the active-patients-to-clinical-support-staff-FTE ratio after an EHR implementation. Our analysis suggests, with a 95% confidence level, that the increase in the number of active patients (P=.006), the increase in the active-patients-to-clinician-FTE ratio (P<.001), and the increase in the clinic net revenue (P<.001) are positively associated with the EHR implementation, likely contributing substantially to an average break-even point of 10 months.
Conclusions: We found that primary care clinics can realize a positive ROI with EHR. Our analysis of the variances in the time required to achieve cost recovery from EHR investments suggests that a positive ROI does not appear automatically upon implementing an EHR and that a clinic's ability to leverage EHR for process changes seems to play a role. Policies that provide support to help primary care practices successfully make EHR-enabled changes, such as support of clinic workflow optimization with an EHR system, could facilitate the realization of positive ROI from EHR in primary care practices.
Keywords: ROI indicator; cost recovery from EHR implementation; physician satisfaction with EHR; primary care practices; return on investment in electronic health records.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hillestad R, Bigelow J, Bower A, Girosi F, Meili R, Scoville R, Taylor R. Can electronic medical record systems transform health care? Potential health benefits, savings, and costs. Heath Affairs. 2005 Sep;24(5):1103–1117. doi: 10.1377/hlthaff.24.5.1103. http://content.healthaffairs.org/content/24/5/1103.full - DOI - PubMed
-
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009 Apr 9;360(15):1477–9. doi: 10.1056/NEJMp0901592. http://www.nejm.org/doi/full/10.1056/nejmp0901592 - DOI - DOI - PubMed
-
- Bates DW. Getting in step: electronic health records and their role in care coordination. J Gen Intern Med. 2010 Mar;25(3):174–6. doi: 10.1007/s11606-010-1252-x. http://link.springer.com/article/10.1007%2Fs11606-010-1252-x?LI=true#page-1 - DOI - PMC - PubMed
-
- Saleem JJ, Flanagan ME, Wilck NR, Demetriades J, Doebbeling BN. The next-generation electronic health record: perspectives of key leaders from the US Department of Veterans Affairs. J Am Med Inform Assoc. 2013 Jun;20(e1):e175–7. doi: 10.1136/amiajnl-2013-001748. http://jamia.bmj.com/content/20/e1/e175.full - DOI - PMC - PubMed
-
- Black AD, Car J, Pagliari C, Anandan C, Cresswell K, Bokun T, McKinstry B, Procter R, Majeed A, Sheik A. The impact of eHealth on the Quality and Safety of Health Care: a Systematic Overview. PLoS Med. 2011;8(1) doi: 10.1371/journal.pmed.1000387. http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.... - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
