

Severe neurologic syndrome associated with Middle East respiratory syndrome corona virus (MERS-CoV)
- PMID: 25600929
- PMCID: PMC4521086
- DOI: 10.1007/s15010-015-0720-y
Severe neurologic syndrome associated with Middle East respiratory syndrome corona virus (MERS-CoV)
Abstract
Background: Since the identification of the first case of infection with the Middle East respiratory syndrome corona virus (MERS-CoV) in Saudi Arabia in June 2012, the number of laboratory-confirmed cases has exceeded 941 cases globally, of which 347 died. The disease presents as severe respiratory infection often with shock, acute kidney injury, and coagulopathy. Recently, we observed three cases who presented with neurologic symptoms. These are so far the first reported cases of neurologic injury associated with MERS-CoV infection.
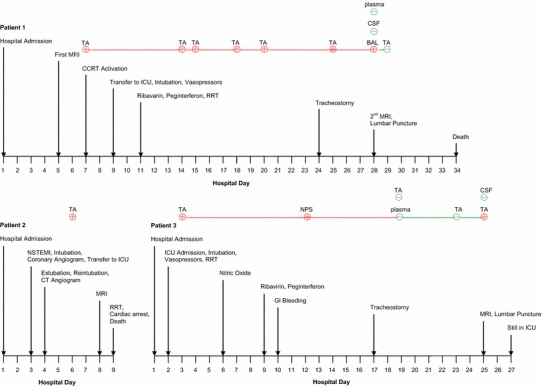
Methods: Data was retrospectively collected from three patients admitted with MERS-CoV infection to Intensive Care unit (ICU) at King Abdulaziz Medical City, Riyadh. They were managed separately in three different wards prior to their admission to ICU.
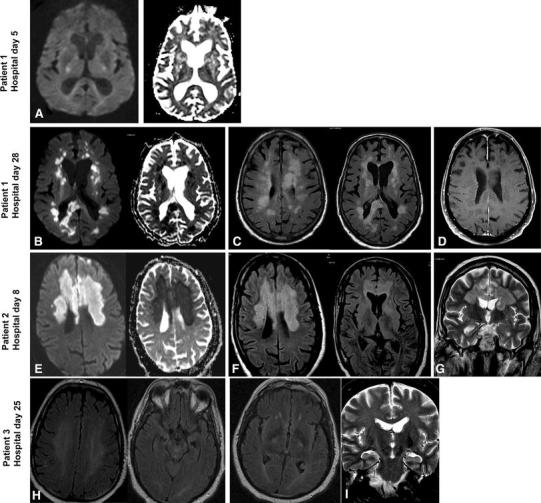
Finding: The three patients presented with severe neurologic syndrome which included altered level of consciousness ranging from confusion to coma, ataxia, and focal motor deficit. Brain MRI revealed striking changes characterized by widespread, bilateral hyperintense lesions on T2-weighted imaging within the white matter and subcortical areas of the frontal, temporal, and parietal lobes, the basal ganglia, and corpus callosum. None of the lesions showed gadolinium enhancement.
Interpretation: CNS involvement should be considered in patients with MERS-CoV and progressive neurological disease, and further elucidation of the pathophysiology of this virus is needed.
Figures
References
-
- Middle East respiratory syndrome coronavirus (MERS-CoV)—update. http://www.who.int/csr/don/26-december-2014-mers/en/. Accessed 15 Jan 2015 - PMC - PubMed
-
- Arabi YM, Arifi AA, Balkhy HH, Najm H, Aldawood AS, Ghabashi A, et al. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;60:389–397. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
