

What can the national quality forum tell us about performance measurement in anesthesiology?
- PMID: 25602454
- PMCID: PMC4350990
- DOI: 10.1213/ANE.0000000000000553
What can the national quality forum tell us about performance measurement in anesthesiology?
Abstract
Background: Anesthesiologists face increasing pressure to demonstrate the value of the care they provide, whether locally or nationally through public reporting and payor requirements. In this article, we describe the current state of performance measurement in anesthesia care at the national level and highlight gaps and opportunities in performance measurement for anesthesiologists.
Methods: We evaluated all endorsed performance measures in the National Quality Forum (NQF), the clearinghouse for all federal performance measures, and classified all measures as follows: (1) anesthesia-specific; (2) surgery-specific; (3) jointly attributable; or (4) other. We used NQF-provided descriptors to characterize measures in terms of (1) structure, process, outcome, or efficiency; (2) patients, disease, and events targeted; (3) procedural specialty; (4) reporting eligibility; (5) measures stewards; and (6) timing in the care stream.
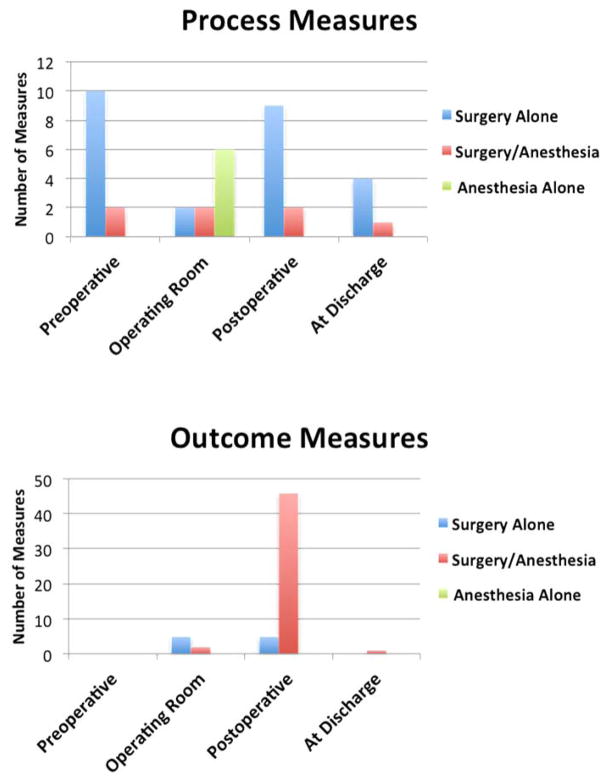
Results: Of the 637 endorsed performance measures, few (6, 1.0%) were anesthesia-specific. An additional 39 measures (6.1%) were surgery-specific, and 67 others (10.5%) were jointly attributable. "Anesthesia-specific" measures addressed preoperative antibiotic timing (n = 4), normothermia (n = 1), and protocol use for the placement of central venous catheter (n = 1). Jointly attributable measures included outcome measures (n = 49/67, 73.1%), which were weighted toward mortality alone (n = 24) and cardiac surgery (n = 14). Other jointly attributable measures addressed orthopedic surgery (n = 4), general surgical oncologic resections (n = 12), or nonspecified surgeries (n = 15), but none specifically addressed anesthesia care outside the operating room such as for endoscopy. Only 4 measures were eligible for value-based purchasing. No named anesthesiology professional groups were among measure stewards, but surgical professional groups (n = 33/67, 47%) were frequent measure stewards.
Conclusions: Few NQF performance measures are specific to anesthesia practice, and none of these appears to demonstrate the value of anesthesia care or differentiate high-quality providers. To demonstrate their role in patient-centered, outcome-driven care, anesthesiologists may consider actively partnering in jointly attributable or team-based reporting. Future measures may incorporate surgical procedures not proportionally represented, as well as procedural and sedation care provided in nonoperating room settings.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- The joint commission recipients of 2007 Ernest Amory Codman awards. National health care award for performance measurement. The Joint Commission Perspectives. 2008 Jan;28(1):3, 10. - PubMed
-
- Pronovost PJ, Demski R, Callender T, Winner L, Miller MR, Austin JM, Berenholtz SM National Leadership Core Measures Work Groups. Demonstrating high reliability on accountability measures at the Johns Hopkins hospital. Jt Comm J Qual Patient Saf. 2013;39(12):531–44. - PubMed
-
- Dimick JB, Ghaferi AA, Osborne NH, Ko CY, Hall BL. Reliability adjustment for reporting hospital outcomes with surgery. Ann Surg. 2012;255(4):703–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
