

Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air
- PMID: 25603202
- PMCID: PMC4704686
- DOI: 10.1097/ALN.0000000000000551
Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air
Abstract
Background: Core temperature patterns in patients warmed with forced air remain poorly characterized. Also unknown is the extent to which transient and mild intraoperative hypothermia contributes to adverse outcomes in broad populations.
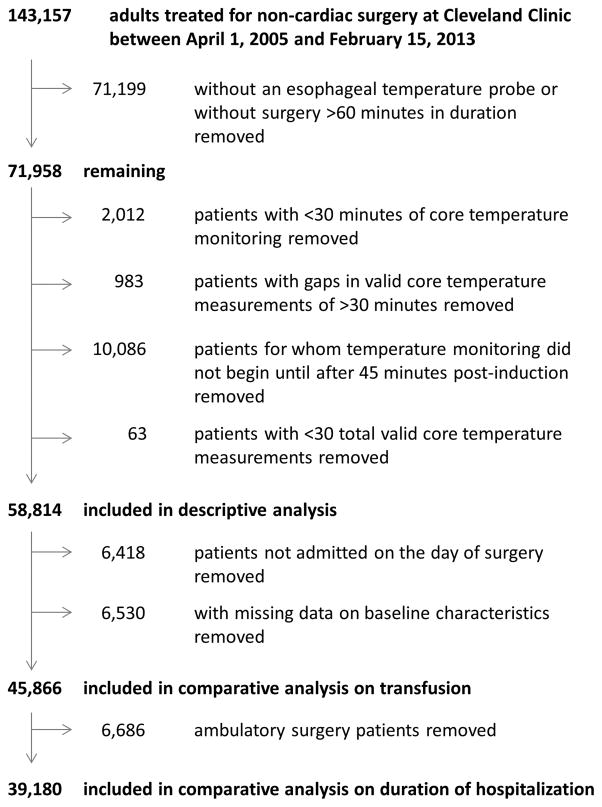
Methods: We evaluated esophageal (core) temperatures in 58,814 adults having surgery lasting >60 min who were warmed with forced air. Independent associations between hypothermic exposure and transfusion requirement and duration of hospitalization were evaluated.
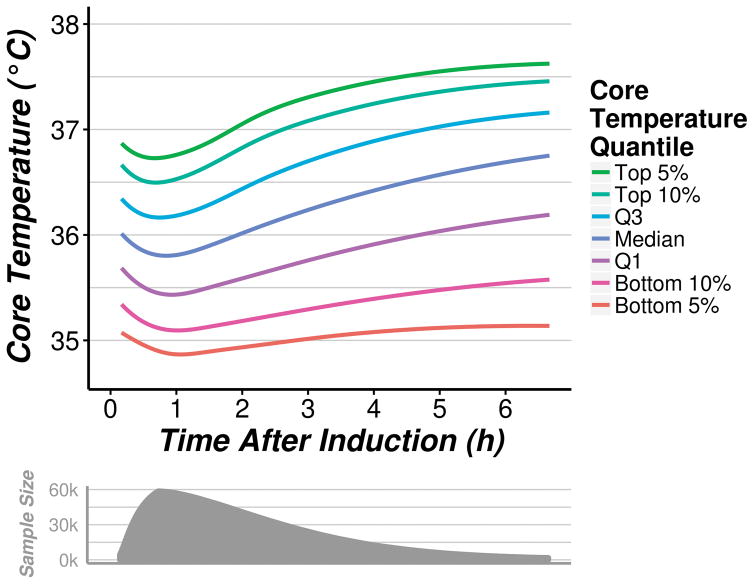
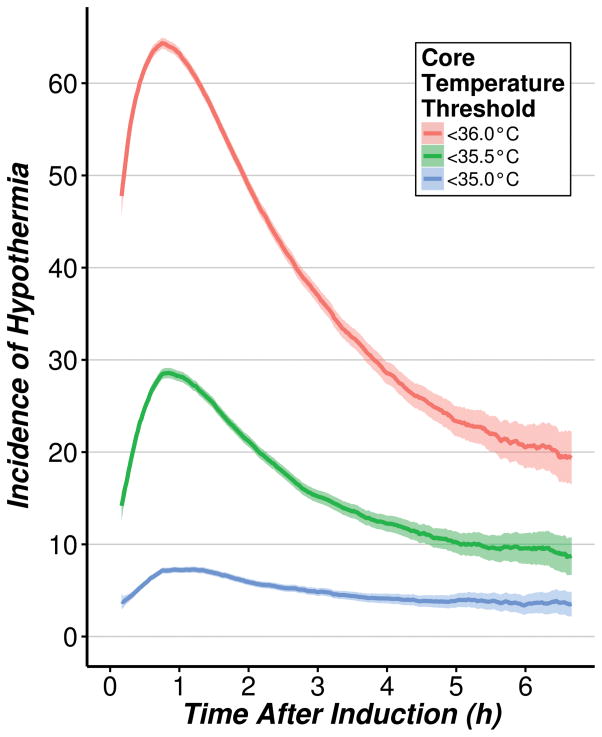
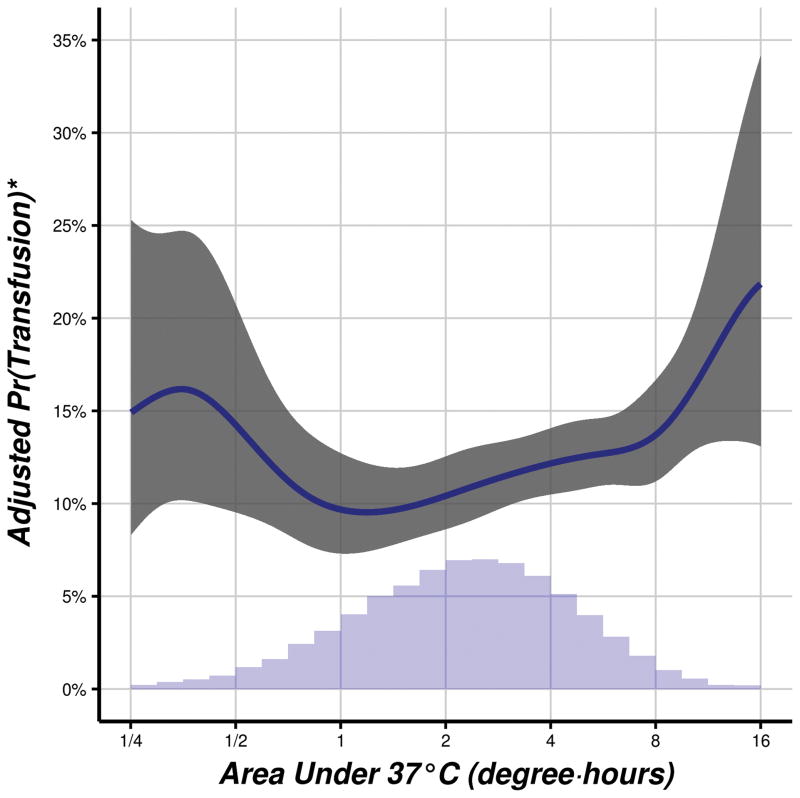
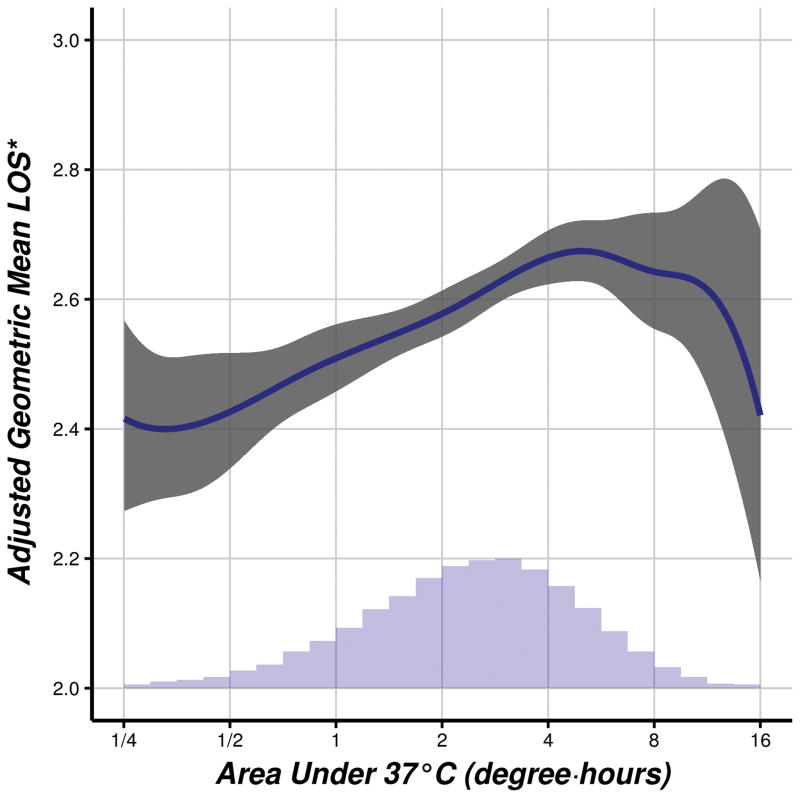
Results: In every percentile subgroup, core temperature decreased during the first hour and subsequently increased. The mean lowest core temperature during the first hour was 35.7 ± 0.6°C. Sixty-four percent of the patients reached a core temperature threshold of <36°C 45 min after induction; 29% reached a core temperature threshold of <35.5°C. Nearly half the patients had continuous core temperatures <36°C for more than an hour, and 20% of the patients were <35.5°C for more than an hour. Twenty percent of patients had continuous core temperatures <36°C for more than 2 h, and 8% of the patients were below 35.5°C for more than 2 h. Hypothermia was independently associated with both transfusions and duration of hospitalization, although the prolongation of hospitalization was small.
Conclusions: Even in actively warmed patients, hypothermia is routine during the first hour of anesthesia. Thereafter, average core temperatures progressively increase. Nonetheless, intraoperative hypothermia was common, and often prolonged. Hypothermia was associated with increased transfusion requirement, which is consistent with numerous randomized trials.
Figures

Comment in
-
Perioperative temperature management: time for a new standard of care?Anesthesiology. 2015 Feb;122(2):229-30. doi: 10.1097/ALN.0000000000000552. Anesthesiology. 2015. PMID: 25603200 No abstract available.
References
-
- Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement: A meta-analysis. Anesthesiology. 2008;108:71–7. - PubMed
-
- Kurz A, Sessler DI, Lenhardt RA. Study of wound infections and temperature group: Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. N Engl J Med. 1996;334:1209–15. - PubMed
-
- Frank SM, Fleisher LA, Breslow MJ, Higgins MS, Olson KF, Kelly S, Beattie C. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events: A randomized clinical trial. JAMA. 1997;277:1127–34. - PubMed
-
- Leslie K, Sessler DI, Bjorksten AR, Moayeri A. Mild hypothermia alters propofol pharmacokinetics and increases the duration of action of atracurium. Anesth Analg. 1995;80:1007–14. - PubMed
-
- Lenhardt R, Marker E, Goll V, Tschernich H, Kurz A, Sessler DI, Narzt E, Lackner F. Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology. 1997;87:1318–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
