

Renal function during long-term lithium treatment: a cross-sectional and longitudinal study
- PMID: 25604586
- PMCID: PMC4300557
- DOI: 10.1186/s12916-014-0249-4
Renal function during long-term lithium treatment: a cross-sectional and longitudinal study
Abstract
Background: The effects of lithium treatment on renal function have been previously shown, albeit with discrepancies regarding their relevance. In this study, we examined glomerular filtration rate in patients treated with lithium for up to 33 years.
Methods: All lithium patients registered from 1980 to 2012 at a Lithium Clinic were screened. Estimated glomerular filtration rate (eGFR) was calculated from serum creatinine concentration using the Modification of Diet in Renal Disease Study Group equation. A cross-sectional evaluation of the last available eGFR of 953 patients was carried out using multivariate regression analysis for gender, current age, and duration of lithium treatment. Survival analysis was subsequently applied to calculate the time on lithium needed to enter the eGFR ranges 45 to 59 mL/min/1.73 m² (G3a) or 30 to 44 mL/min/1.73 m² (G3b). Finally, 4-year follow-up of eGFR was examined in subgroups of patients who, after reduction to an eGFR lower than 45 mL/min/1.73 m² either i) continued lithium at the same therapeutic range or ii) discontinued lithium or continued at concentrations below the therapeutic range (0.5 mmol/L).
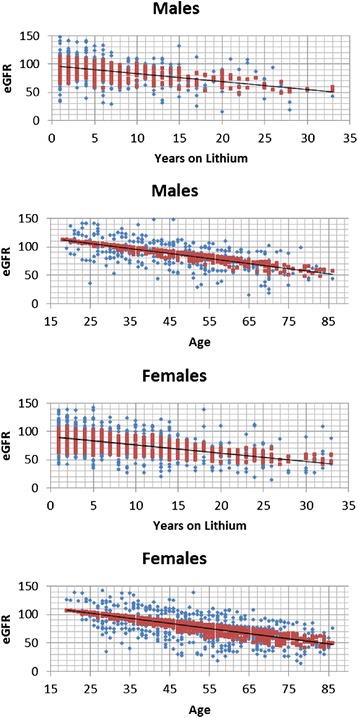
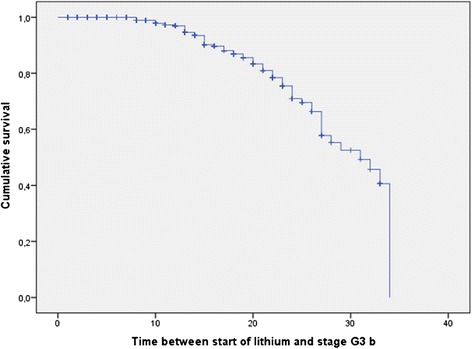
Results: In the cross-sectional evaluation, eGFR was found to be lower in women (by 3.47 mL/min/1.73 m²), in older patients (0.73 mL/min/1.73 m² per year of age), and in patients with longer lithium treatment (0.73 mL/min/1.73 m² per year). Half of the patients treated for longer than 20 years had an eGFR lower than 60 mL/min/1.73 m². The median time on lithium taken to enter G3a or G3b was 25 years (95% CI, 23.2-26.9) and 31 years (95% CI, 26.6-35.4), respectively. Progression of renal failure throughout the 4-year follow-up after a reduction to an eGFR lower than 45 mL/min/1.73 m² did not differ between the subgroup who continued lithium as before and the subgroup who either discontinued lithium or continued at concentrations below the therapeutic range.
Conclusions: Duration of lithium treatment is to be added to advancing age as a risk factor for reduced glomerular filtration rate. However, renal dysfunction tends to appear after decades of treatment and to progress slowly and irrespective of lithium continuation.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
