

Intensity-modulated proton therapy for elective nodal irradiation and involved-field radiation in the definitive treatment of locally advanced non-small-cell lung cancer: a dosimetric study
- PMID: 25604729
- PMCID: PMC4410064
- DOI: 10.1016/j.cllc.2014.12.001
Intensity-modulated proton therapy for elective nodal irradiation and involved-field radiation in the definitive treatment of locally advanced non-small-cell lung cancer: a dosimetric study
Abstract
Background: Photon involved-field (IF) radiation therapy (IFRT), the standard for locally advanced (LA) non-small cell lung cancer (NSCLC), results in favorable outcomes without increased isolated nodal failures, perhaps from scattered dose to elective nodal stations. Because of the high conformality of intensity-modulated proton therapy (IMPT), proton IFRT could increase nodal failures. We investigated the feasibility of IMPT for elective nodal irradiation (ENI) in LA-NSCLC.
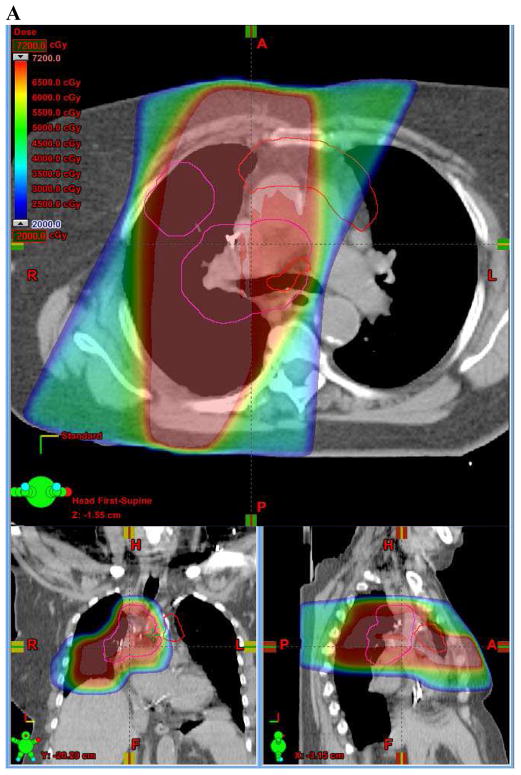
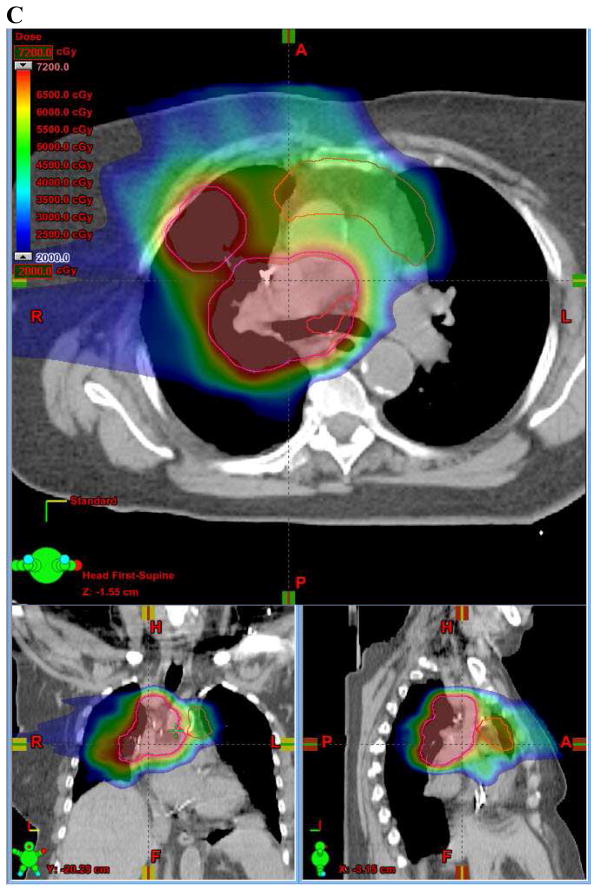
Patients and methods: IMPT IFRT plans were generated to the same total dose of 66.6-72 Gy received by 20 LA-NSCLC patients treated with photon IFRT. IMPT ENI plans were generated to 46 cobalt Gray equivalent (CGE) to elective nodal planning treatment volumes (PTV) plus 24 CGE to IF-PTVs.
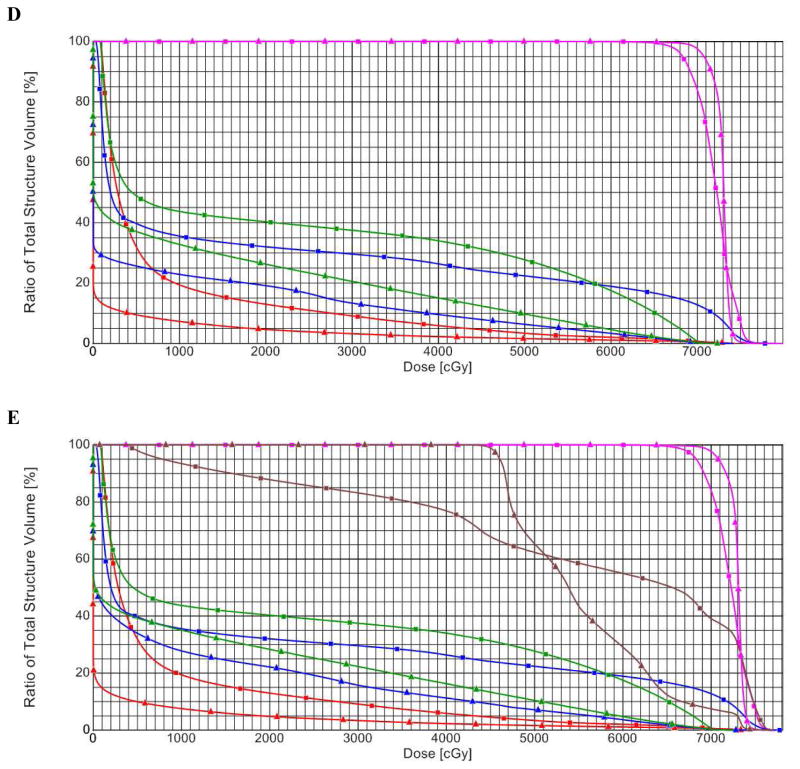
Results: Proton IFRT and ENI improved the IF-PTV percentage of volume receiving 95% of the prescribed dose (D95) by 4% (P < .01) compared with photon IFRT. All evaluated dosimetric parameters improved significantly with both proton plans. The lung percentage of volume receiving 20 Gy/CGE (V20) and mean lung dose decreased 18% (P < .01) and 36% (P < .01), respectively, with proton IFRT, and 11% (P = .03) and 26% (P < .01) with ENI. The mean esophagus dose decreased 16% with IFRT and 12% with ENI; heart V25 decreased 63% with both (all P < .01).
Conclusion: This study demonstrates the feasibility of IMPT for LA-NSCLC ENI. Potential decreased toxicity indicates that IMPT could allow ENI while maintaining a favorable therapeutic ratio compared with photon IFRT.
Keywords: ENI; IFRT; IMPT; NSCLC; Radiation therapy.
Published by Elsevier Inc.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Edge SB. AJCC cancer staging manual. 7. New York: Springer; 2010. American Joint Committee on Cancer. - PubMed
-
- Furuse K, Fukuoka M, Kawahara M, et al. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. J Clin Oncol. 1999 Sep;17(9):2692–2699. - PubMed
-
- Curran WJ., Jr Evolving chemoradiation treatment strategies for locally advanced non-small-cell lung cancer. Oncology (Williston Park) 2003 Dec;17(12 Suppl 13):7–14. - PubMed
-
- Fournel P, Robinet G, Thomas P, et al. Randomized phase III trial of sequential chemoradiotherapy compared with concurrent chemoradiotherapy in locally advanced non-small-cell lung cancer: Groupe Lyon-Saint-Etienne d’Oncologie Thoracique-Groupe Francais de Pneumo-Cancerologie NPC 95-01 Study. J Clin Oncol. 2005 Sep 1;23(25):5910–5917. - PubMed
-
- Rengan R, Rosenzweig KE, Venkatraman E, et al. Improved local control with higher doses of radiation in large-volume stage III non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004 Nov 1;60(3):741–747. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
