

Examination of autoantibody status and clinical features associated with cancer risk and cancer-associated scleroderma
- PMID: 25605296
- PMCID: PMC4400658
- DOI: 10.1002/art.39022
Examination of autoantibody status and clinical features associated with cancer risk and cancer-associated scleroderma
Abstract
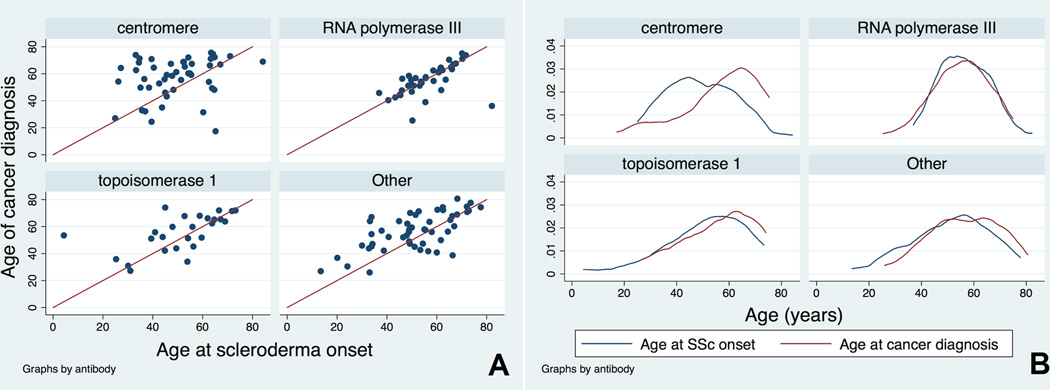
Objective: We previously reported a contemporaneous onset of cancer and scleroderma in patients with anti-RNA polymerase III antibodies, and we identified a biologic link between cancer and scleroderma. This investigation was designed to further evaluate whether autoantibody status and other characteristics are associated with cancer and a clustering of cancer with scleroderma onset.
Methods: Logistic regression analysis was performed to assess the relationship of 2 outcomes, cancer (model 1) and a short (±2 years) cancer-scleroderma interval (model 2), with autoantibody status and scleroderma covariates.
Results: Of 1,044 scleroderma patients, 168 (16.1%) had cancer. In the adjusted model 1, only older age at scleroderma onset (odds ratio 1.04 [95% confidence interval 1.02-1.05]) and white race (odds ratio 2.71 [95% confidence interval 1.22-6.04]) were significantly associated with an increased overall risk of cancer. In the adjusted model 2, only anti-RNA polymerase III positivity (odds ratio 5.08 [95% confidence interval 1.60-16.1]) and older age at scleroderma onset (odds ratio 1.04 [95% confidence interval 1.00-1.08]) were significantly associated with a short cancer-scleroderma interval. While anti-RNA polymerase III positivity was associated with a short cancer-scleroderma interval independent of age at scleroderma onset, the cancer-scleroderma interval shortened with older age at scleroderma onset in other antibody groups (Spearman's correlation P < 0.05), particularly among patients with anti-topoisomerase I antibodies and patients who were negative for anticentromere, anti-topoisomerase I, and anti-RNA polymerase III antibodies.
Conclusion: Increased age at scleroderma onset is strongly associated with cancer risk overall. While anti-RNA polymerase III status is an independent marker of coincident cancer and scleroderma at any age, a clustering of cancer with scleroderma is also seen in patients with anti-topoisomerase I and other autoantibody specificities who develop scleroderma at older ages.
Copyright © 2015 by the American College of Rheumatology.
Conflict of interest statement
Figures
References
-
- Olesen AB, Svaerke C, Farkas DK, Sorensen HT. Systemic sclerosis and the risk of cancer: a nationwide population-based cohort study. The British journal of dermatology. 2010;163(4):800–806. - PubMed
-
- Buchbinder R, Forbes A, Hall S, Dennett X, Giles G. Incidence of malignant disease in biopsy-proven inflammatory myopathy. A population-based cohort study. Annals of internal medicine. 2001;134(12):1087–1095. - PubMed
-
- Hill CL, Zhang Y, Sigurgeirsson B, Pukkala E, Mellemkjaer L, Airio A, et al. Frequency of specific cancer types in dermatomyositis and polymyositis: a population-based study. Lancet. 2001;357(9250):96–100. - PubMed
-
- Zantos D, Zhang Y, Felson D. The overall and temporal association of cancer with polymyositis and dermatomyositis. The Journal of rheumatology. 1994;21(10):1855–1859. - PubMed
-
- Launay D, Le Berre R, Hatron PY, Peyrat JP, Hachulla E, Devulder B, et al. Association between systemic sclerosis and breast cancer: eight new cases and review of the literature. Clinical rheumatology. 2004;23(6):516–522. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
