

Perioperative blood transfusion as a poor prognostic factor after aggressive surgical resection for hilar cholangiocarcinoma
- PMID: 25605416
- PMCID: PMC4412428
- DOI: 10.1007/s11605-014-2741-8
Perioperative blood transfusion as a poor prognostic factor after aggressive surgical resection for hilar cholangiocarcinoma
Abstract
Background: Blood transfusion is linked to a negative outcome for malignant tumors. The aim of this study was to evaluate aggressive surgical resection for hilar cholangiocarcinoma (HCCA) and assess the impact of perioperative blood transfusion on long-term survival.
Methods: Sixty-six consecutive major hepatectomies with en bloc resection of the caudate lobe and extrahepatic bile duct for HCCA were performed using macroscopically curative resection at our institute from 2002 to 2012. Clinicopathologic factors for recurrence and survival were retrospectively assessed.
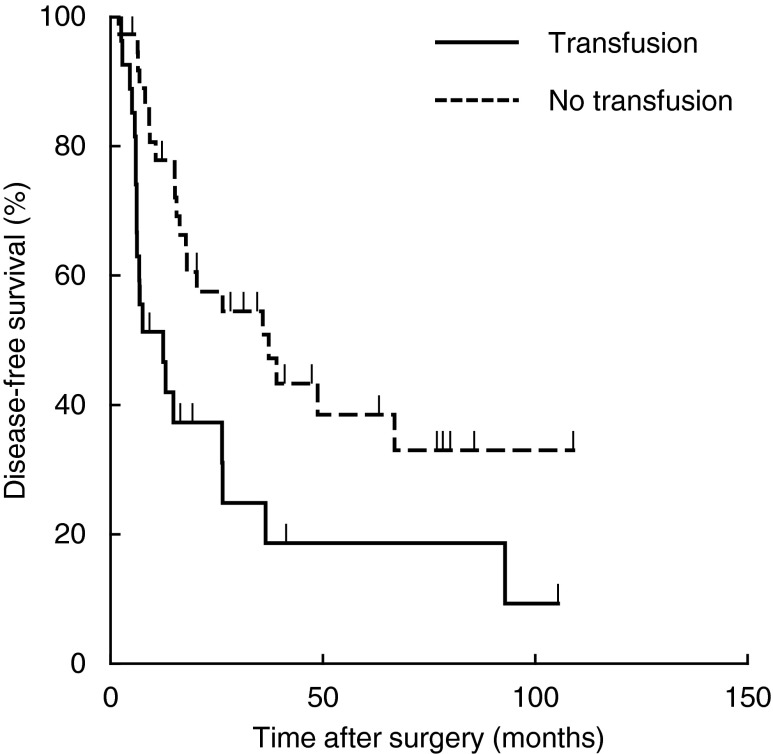
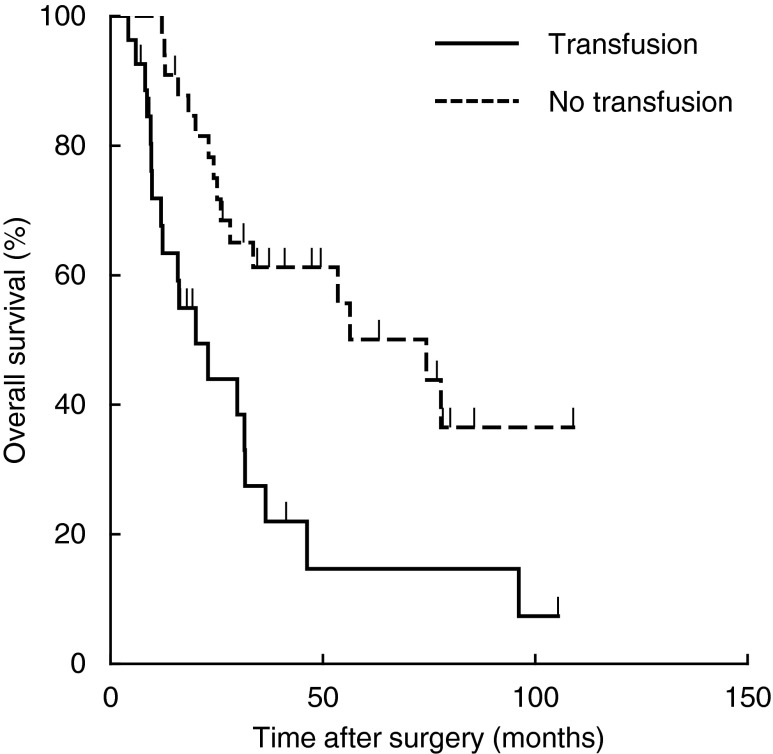
Results: Overall survival rates at 1, 3, and 5 years were 86.7, 47.3, and 35.7 %, respectively. In univariate analysis, perioperative blood transfusion and a histological positive margin were two of several variables found to be significant prognostic factors for recurrence or survival (P<0.05). In multivariate analysis, only perioperative blood transfusion was independently associated with recurrence (hazard ratio (HR)=2.839 (95 % confidence interval (CI), 1.370-5.884), P=0.005), while perioperative blood transfusion (HR=3.383 (95 % CI, 1.499-7.637), P=0.003) and R1 resection (HR=3.125 (95 % CI, 1.025-9.530), P=0.045) were independent risk factors for poor survival.
Conclusions: Perioperative blood transfusion is a strong predictor of poor survival after radical hepatectomy for HCCA. We suggest that circumvention of perioperative blood transfusion can play an important role in long-term survival for patients with HCCA.
Figures
Comment in
-
Perioperative blood transfusion and long-term outcomes after resection of hilar cholangiocarcinoma.J Gastrointest Surg. 2015 Jun;19(6):1192-3. doi: 10.1007/s11605-015-2822-3. Epub 2015 Apr 21. J Gastrointest Surg. 2015. PMID: 25895978 No abstract available.
-
Perioperative blood transfusion as a poor prognostic factor after aggressive surgical resection for hilar cholangiocarcinoma.J Gastrointest Surg. 2015 Jun;19(6):1194-5. doi: 10.1007/s11605-015-2823-2. Epub 2015 Apr 21. J Gastrointest Surg. 2015. PMID: 25895979 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
