

Chikungunya viral arthritis in the United States: a mimic of seronegative rheumatoid arthritis
- PMID: 25605621
- PMCID: PMC4591551
- DOI: 10.1002/art.39027
Chikungunya viral arthritis in the United States: a mimic of seronegative rheumatoid arthritis
Abstract
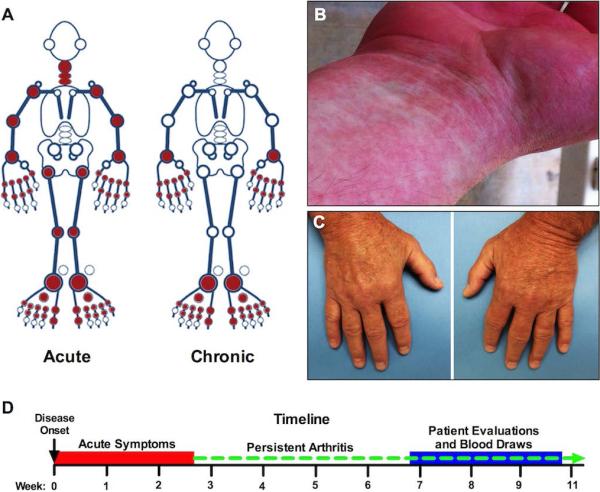
Objective: Chikungunya virus (CHIKV) is an arthritogenic mosquito-transmitted alphavirus that spread to the Caribbean in 2013 and to the US in 2014. CHIKV-infected patients develop inflammatory arthritis that can persist for months or years, but little is known about the rheumatologic and immunologic features of CHIKV-related arthritis in humans, particularly as compared to rheumatoid arthritis (RA). The purpose of this study was to describe these features in a group of 10 American travelers who were nearly simultaneously infected while visiting Haiti in June 2014.
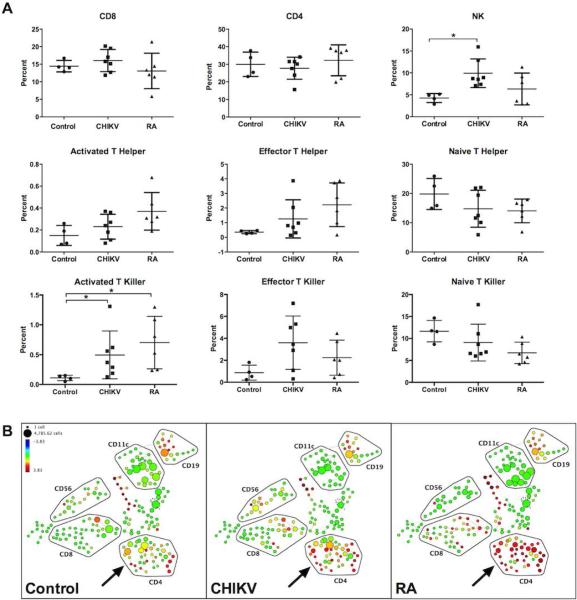
Methods: Patient history was obtained and physical examination and laboratory tests were performed. All patients with CHIKV-related arthritis had detectable levels of anti-CHIKV IgG. Using cytometry by time-of-flight (CyTOF), we analyzed peripheral blood mononuclear cells in CHIKV-infected patients, healthy controls, and patients with untreated, active RA.
Results: Among 10 CHIKV-infected individuals, 8 developed persistent symmetric polyarthritis that met the American College of Rheumatology/European League Against Rheumatism 2010 criteria for (seronegative) RA. CyTOF analysis revealed that RA and CHIKV-infected patients had greater percentages of activated and effector CD4+ and CD8+ T cells than healthy controls.
Conclusion: In addition to similar clinical features, patients with CHIKV infection and patients with RA develop very similar peripheral T cell phenotypes. These overlapping clinical and immunologic features highlight a need for rheumatologists to consider CHIKV infection when evaluating patients with new, symmetric polyarthritis.
© 2015, American College of Rheumatology.
Figures
References
-
- Staples JE, Breiman RF, Powers AM. Chikungunya Fever: An Epidemiological Review of a Re-Emerging Infectious Disease. Clinical Infectious Diseases. 2009;49(6):942–8. - PubMed
-
- Enserink M. Crippling Virus Set to Conquer Western Hemisphere. Science. 2014;344(6185):678–9. - PubMed
-
- Kuehn BM. Chikungunya virus transmission found in the united states: Us health authorities brace for wider spread. JAMA. 2014;312(8):776–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
