

Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia
- PMID: 25605628
- PMCID: PMC5024022
- DOI: 10.1002/bjs.9764
Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia
Abstract
Background: The optimal surgical approach for treatment of oesophagogastric junction (OGJ) cancer is controversial. A randomized clinical trial (JCOG9502) comparing transhiatal (TH) and left thoracoabdominal (LTA) approaches was stopped after the first interim analysis owing to limited efficacy for LTA resections. Complete 10-year follow-up data are now available.
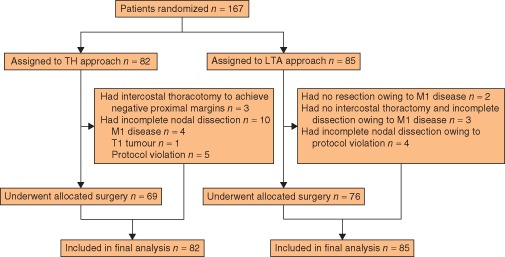
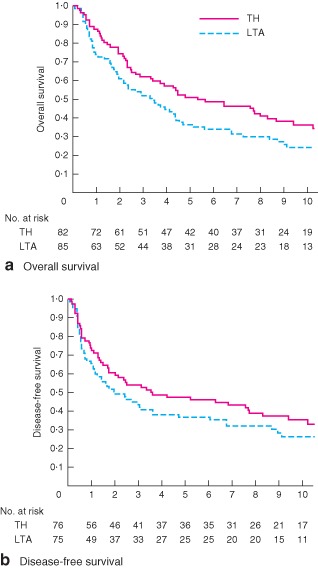
Methods: Patients with histologically proven adenocarcinoma of the OGJ or gastric cardia with oesophageal invasion of 3 cm or less were randomized to a TH or LTA approach. Both groups underwent total gastrectomy and splenectomy with D2 nodal dissection plus para-aortic lymphadenectomy above the left renal vein. For LTA, a thorough mediastinal lymphadenectomy below the left inferior pulmonary vein was also mandatory. The primary endpoint was overall survival.
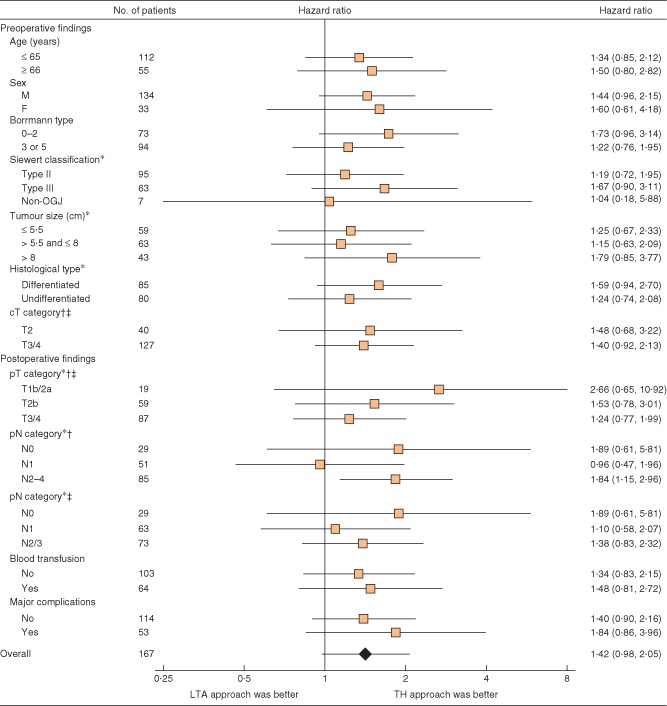
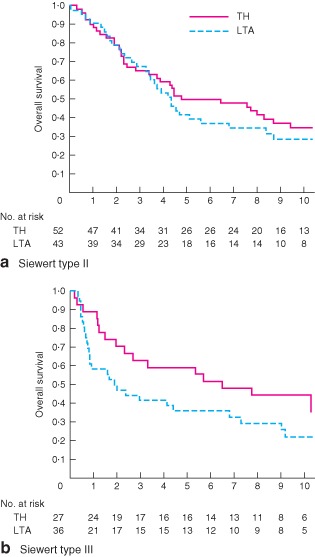
Results: A total of 167 patients (82 TH, 85 LTA) were enrolled. The 10-year overall survival rate was 37 (95 per cent c.i. 26 to 47) per cent for the TH approach and 24 (15 to 34) per cent for the LTA technique (P = 0·060). The hazard ratio for death was 1·42 (0·98 to 2·05) for the LTA technique. Subgroup analysis based on the Siewert classification indicated non-significant survival advantages in favour of the TH approach.
Conclusion: LTA resections should be avoided in the treatment of adenocarcinoma of the OGJ or gastric cardia.
Registration number: NCT00149266 (https://www.clinicaltrials.gov).
© 2015 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Comment in
-
A commentary on "Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia".Transl Gastroenterol Hepatol. 2016 Mar 16;1:12. doi: 10.21037/tgh.2016.03.08. eCollection 2016. Transl Gastroenterol Hepatol. 2016. PMID: 28138579 Free PMC article. No abstract available.
References
-
- Devesa SS, Blot WJ, Fraumeni JF Jr . Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998; 83: 2049–2053. - PubMed
-
- Bollschweiler E, Wolfgarten E, Gutschow C, Hölscher AH. Demographic variations in the rising incidence of esophageal adenocarcinoma in white males. Cancer 2001; 92: 549–555. - PubMed
-
- Hulscher JB, Tijssen JG, Obertop H, van Lanschot JJ. Transthoracic versus transhiatal resection for carcinoma of the esophagus: a meta‐analysis. Ann Thorac Surg 2001; 72: 306–313. - PubMed
-
- Siewert JR, Stein HJ. Carcinoma of the gastroesophageal junction: classification, pathology and extent of resection. Dis Esoph 1996; 9: 173–182.
-
- Kodera Y, Yamamura Y, Shimizu Y, Torii A, Hirai T, Yasui K et al Adenocarcinoma of the gastroesophageal junction in Japan: relevance of Siewert's classification applied to 177 cases resected at a single institution. J Am Coll Surg 1999; 189: 594–601. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
