

RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation
- PMID: 25605856
- PMCID: PMC4334775
- DOI: 10.1200/JCO.2014.57.9029
RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation
Erratum in
-
ERRATA.J Clin Oncol. 2015 Sep 10;33(26):2934. doi: 10.1200/JCO.2015.64.1290. J Clin Oncol. 2015. PMID: 26355145 Free PMC article. No abstract available.
Abstract
Purpose: The Radiation Therapy Oncology Group 9804 study identified good-risk patients with ductal carcinoma in situ (DCIS), a breast cancer diagnosis found frequently in mammographically detected cancers, to test the benefit of radiotherapy (RT) after breast-conserving surgery compared with observation.
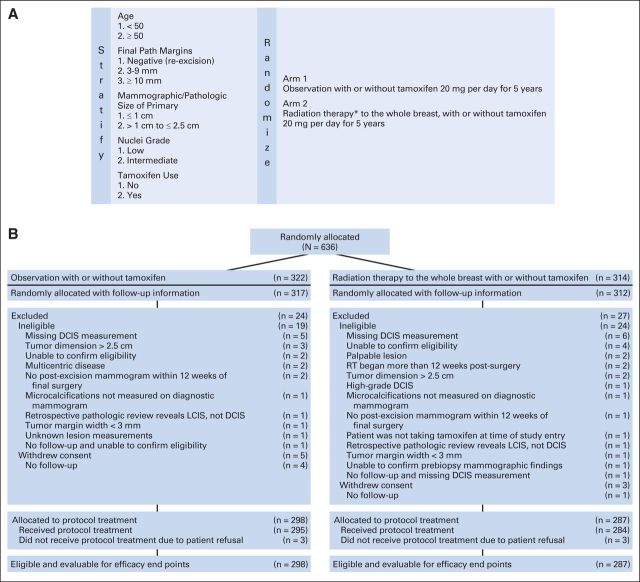
Patients and methods: This prospective randomized trial (1998 to 2006) in women with mammographically detected low- or intermediate-grade DCIS, measuring less than 2.5 cm with margins ≥ 3 mm, compared RT with observation after surgery. The study was designed for 1,790 patients but was closed early because of lower than projected accrual. Six hundred thirty-six patients from the United States and Canada were entered; tamoxifen use (62%) was optional. Ipsilateral local failure (LF) was the primary end point; LF and contralateral failure were estimated using cumulative incidence, and overall and disease-free survival were estimated using the Kaplan-Meier method.
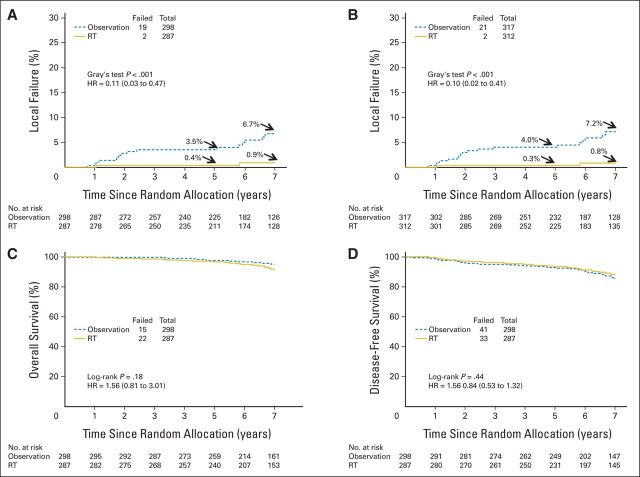
Results: Median follow-up time was 7.17 years (range, 0.01 to 11.33 years). Two LFs occurred in the RT arm, and 19 occurred in the observation arm. At 7 years, the LF rate was 0.9% (95% CI, 0.0% to 2.2%) in the RT arm versus 6.7% (95% CI, 3.2% to 9.6%) in the observation arm (hazard ratio, 0.11; 95% CI, 0.03 to 0.47; P < .001). Grade 1 to 2 acute toxicities occurred in 30% and 76% of patients in the observation and RT arms, respectively; grade 3 or 4 toxicities occurred in 4.0% and 4.2% of patients, respectively. Late RT toxicity was grade 1 in 30%, grade 2 in 4.6%, and grade 3 in 0.7% of patients.
Conclusion: In this good-risk subset of patients with DCIS, with a median follow-up of 7 years, the LF rate was low with observation but was decreased significantly with the addition of RT. Longer follow-up is planned because the timeline for LF in this setting seems protracted.
Trial registration: ClinicalTrials.gov NCT00003857.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
[Radiotherapy also for good-risk ductal carcinoma in situ? Results from a prospective randomized RTOG trial].Strahlenther Onkol. 2015 Jun;191(6):536-8. doi: 10.1007/s00066-015-0836-0. Strahlenther Onkol. 2015. PMID: 26221647 German. No abstract available.
-
[Adjuvant radiotherapy significantly also reduces local recurrence rate for prognostically favorable DCIS].Strahlenther Onkol. 2015 Dec;191(12):997-1000. doi: 10.1007/s00066-015-0906-3. Strahlenther Onkol. 2015. PMID: 26497497 German. No abstract available.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–1241. - PubMed
-
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347:1227–1232. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: Findings from the National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16:441–452. - PubMed
-
- Julien JP, Bijker N, Fentimen IS, et al. Radiotherapy in breast conserving treatment for ductal carcinoma in situ: First results of the EORTC randomized phase III trial 10853—EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. Lancet. 2000;355:528–533. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
