

Muscle metastases: comparison of features in different primary tumours
- PMID: 25608474
- PMCID: PMC4331826
- DOI: 10.1186/1470-7330-14-21
Muscle metastases: comparison of features in different primary tumours
Abstract
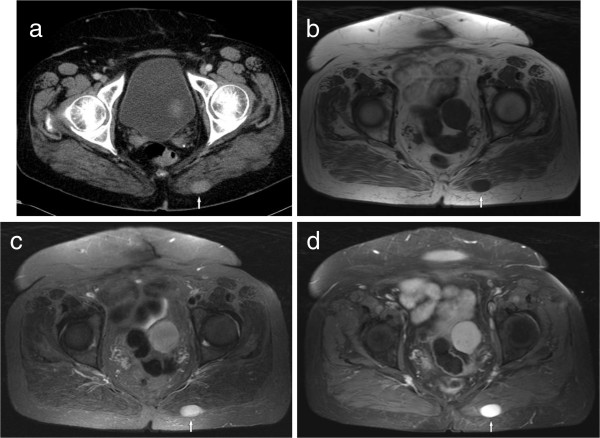
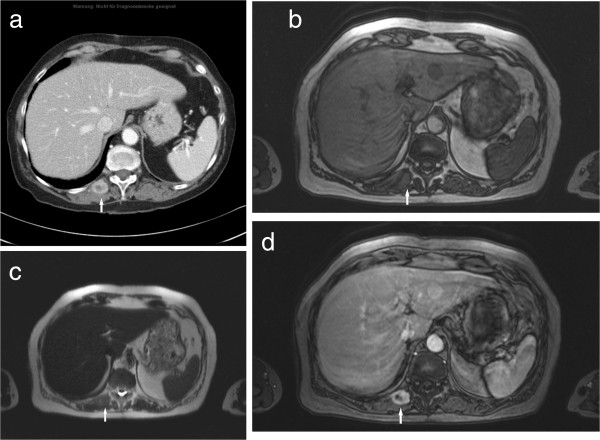
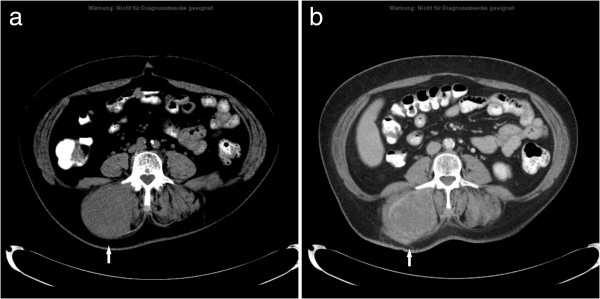
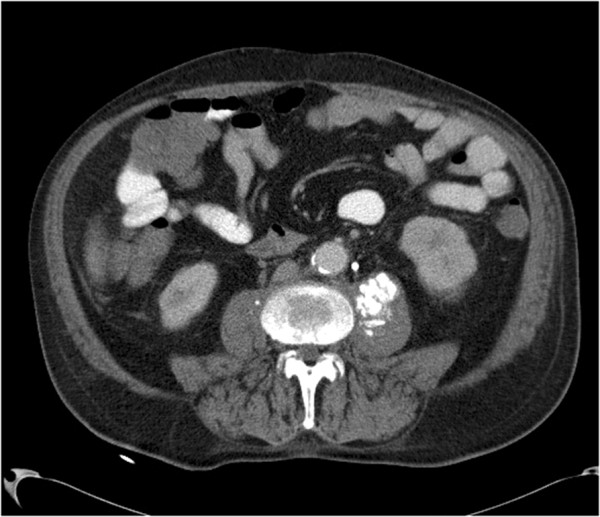
Background: Muscle metastases (MM) from solid tumours are rare. The aim of this study was to describe radiological features of MM, and to compare their patterns in different malignancies.
Methods: A retrospective search in the statistical database of our institution revealed 61 cases of MM. Additionally, a retrospective search in Pubmed database was performed. Together with our cases the present analysis comprises 461 patients (682 MM).
Results: MM derived from the following malignancies: lung cancer (25.1%), gastrointestinal tumours (21.0%), and urological tumours (13.2%). Other neoplasias with MM were rare. MM were localised most frequently in the thigh muscles, the extraocular musculature, and the gluteal and paravertebral muscles. The localisation of MM was different in several primary malignancies.
Conclusion: MM present with a broad spectrum of radiological features. Different CT imaging findings of MM were observed in different primary tumours. The localisation of MM also varies with different primary malignancies.
Figures


References
-
- Acinas Garcia O, Fernandez FA, Satue EG, Buelta L, Val-Bernal JF. Metastasis of malignant neoplasms to skeletal muscle. Rev Esp Oncol. 1984;31:57–67. - PubMed
-
- Willis RA. The Spread of Tumours in the Human Body. London: Butterworth; 1952.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
