

Imaging of malignancies of the biliary tract- an update
- PMID: 25608662
- PMCID: PMC4331820
- DOI: 10.1186/1470-7330-14-14
Imaging of malignancies of the biliary tract- an update
Abstract
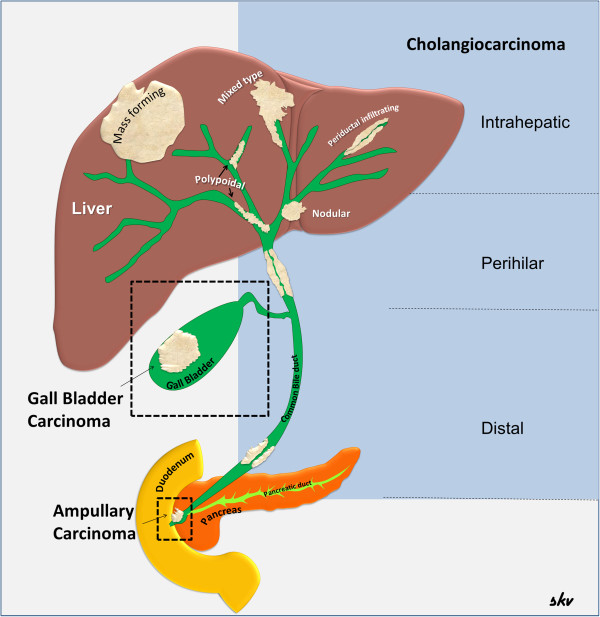
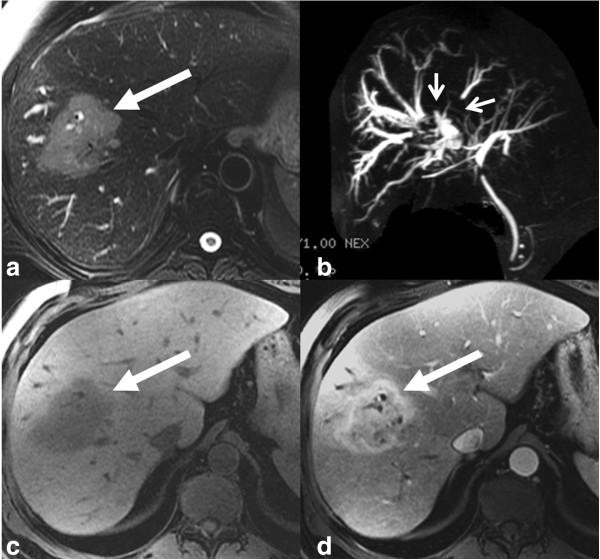
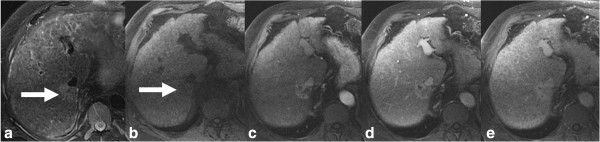
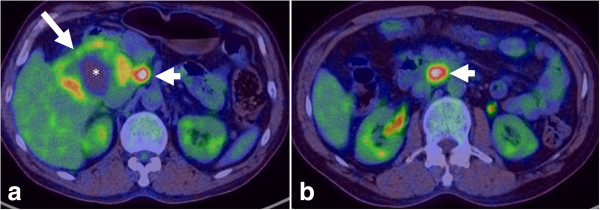
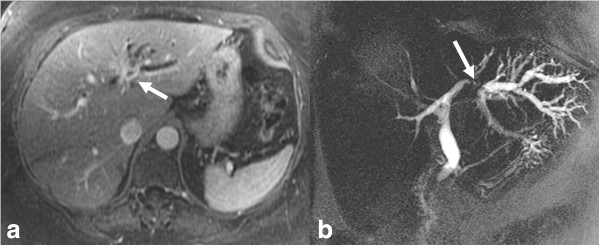
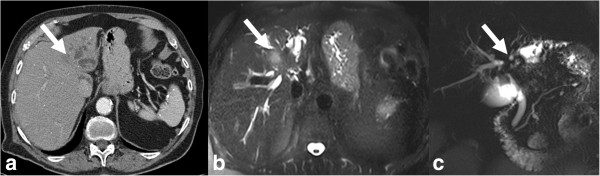
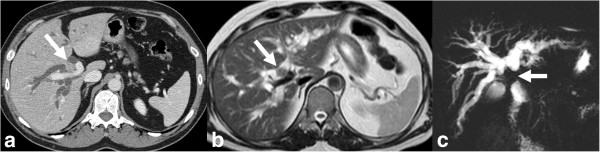
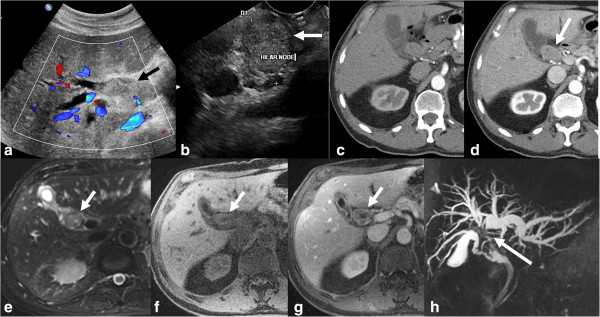
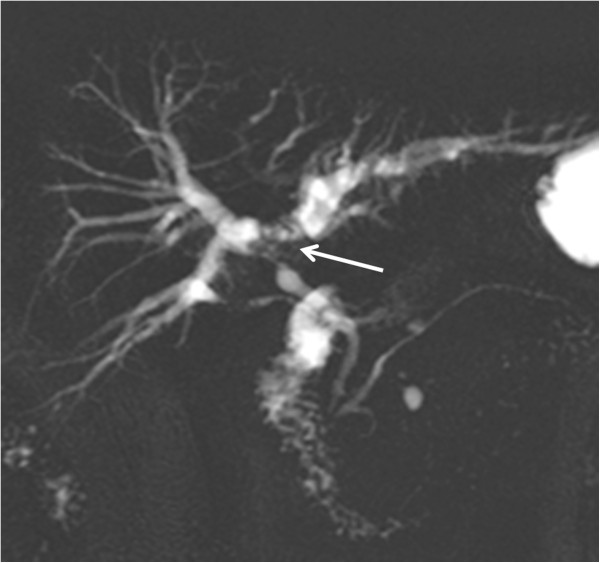
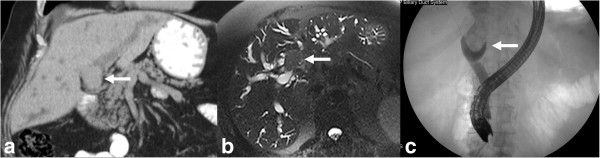
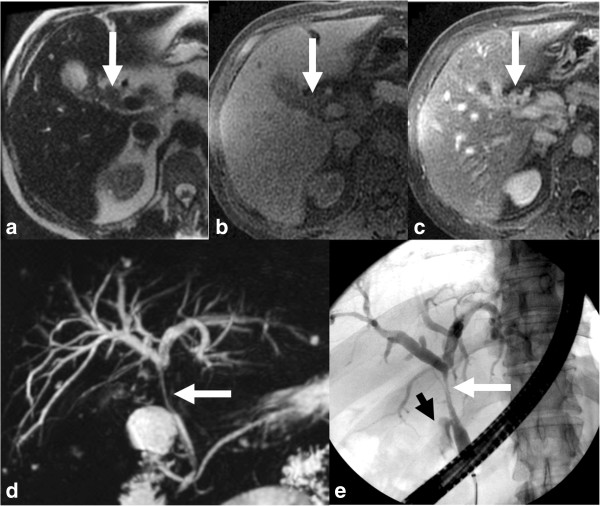
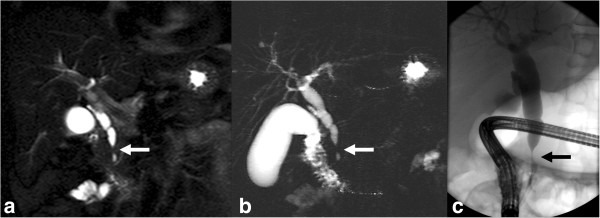
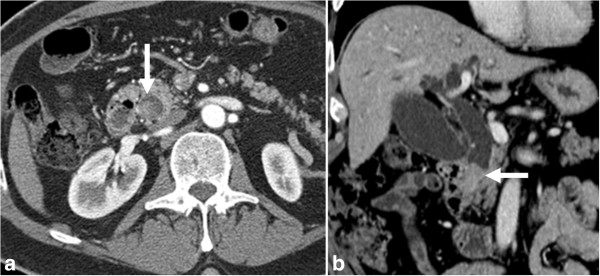
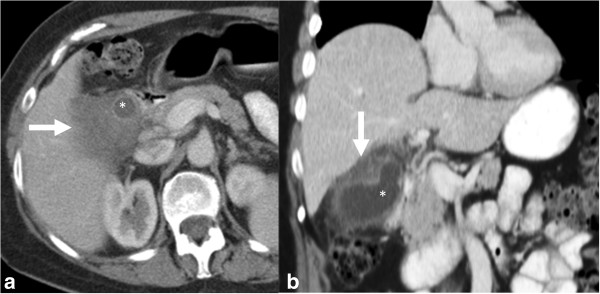
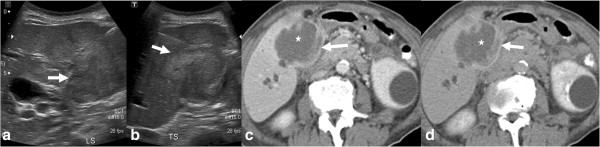
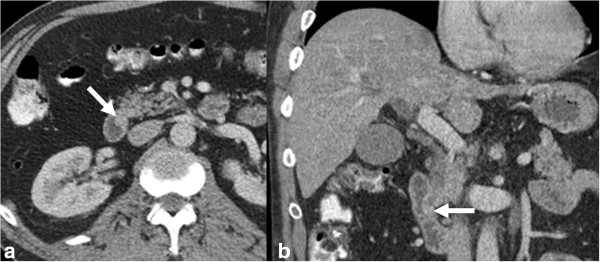
Malignancies of the biliary tract include cholangiocarcinoma, gallbladder cancers and carcinoma of the ampulla of Vater. Biliary tract adenocarcinomas are the second most common primary hepatobiliary cancer. Due to their slow growing nature, non-specific and late symptomatology, these malignancies are often diagnosed in advanced stages with poor prognosis. Apart from incidental discovery of gall bladder carcinoma upon cholecystectomy, early stage biliary tract cancers are now detected with computed tomography (CT) and magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatography (MRCP). Accurate characterization and staging of these indolent cancers will determine outcome as majority of the patients' are inoperable at the time of presentation. Ultrasound is useful for initial evaluation of the biliary tract and gallbladder masses and in determining the next suitable modality for further evaluation. Multimodality imaging plays an integral role in the management of the biliary tract malignancies. The imaging techniques most useful are MRI with MRCP, endoscopic retrograde cholangiopancreatography (ERCP), endoscopic ultrasound (EUS) and positron emission tomography (PET). In this review we will discuss epidemiology and the role of imaging in detection, characterization and management of the biliary tract malignancies under the three broad categories of cholangiocarcinomas (intra- and extrahepatic), gallbladder cancers and ampullary carcinomas.
Figures

References
-
- Craig JR, Peters RL, Edmondson HA. Atlas of Tumor Pathology. 2nd series. Fascicle 26. Washington, D.C: Armed Forces Institute of Pathology; 1989. Tumors of the liver and intrahepatic bile ducts.
-
- Mukhopadhyay S, Landas SK. Putative precursors of gallbladder dysplasia: a review of 400 routinely resected specimens. Arch Pathol Lab Med. 2005;129:386–390. - PubMed
-
- Adsay NV, Klimstra DS. In: Surgical pathology of the GI tract, liver, biliary tract and pancreas. 2. Odze RD, Goldblum JR, editor. Philadelphia, PA: Saunders Elsevier; 2009. Benign and malignant tumors of the gallbladder and extrahepatic biliary tree; pp. 845–875.
-
- Katabi N. Neoplasia of gallbladder and biliary epithelium. Arch Pathol Lab Med. 2010;134:1621–1627. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
