

A neuroprosthesis for control of seated balance after spinal cord injury
- PMID: 25608888
- PMCID: PMC4326199
- DOI: 10.1186/1743-0003-12-8
A neuroprosthesis for control of seated balance after spinal cord injury
Abstract
Background: A major desire of individuals with spinal cord injury (SCI) is the ability to maintain a stable trunk while in a seated position. Such stability is invaluable during many activities of daily living (ADL) such as regular work in the home and office environments, wheelchair propulsion and driving a vehicle. Functional neuromuscular stimulation (FNS) has the ability to restore function to paralyzed muscles by application of measured low-level currents to the nerves serving those muscles.
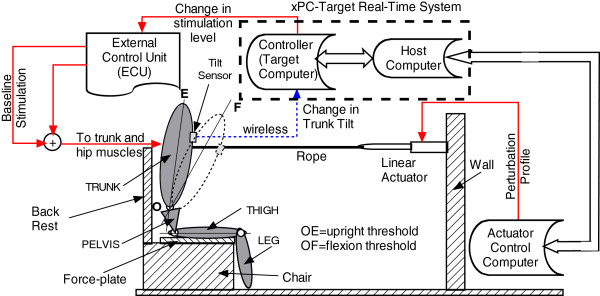
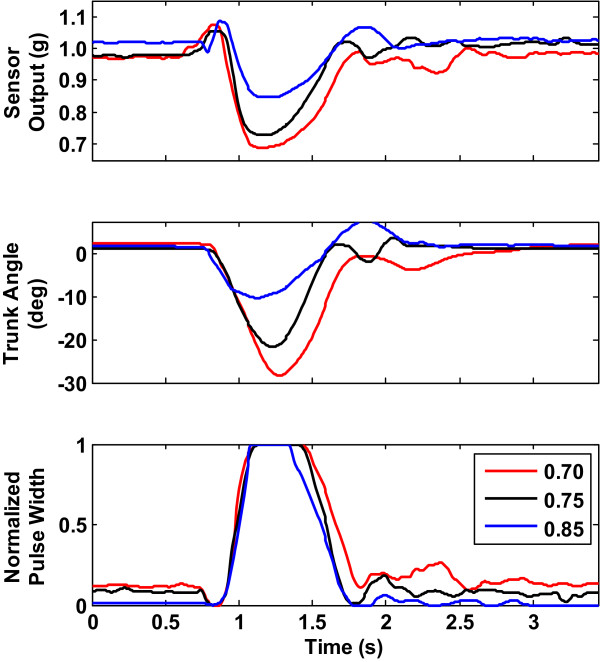
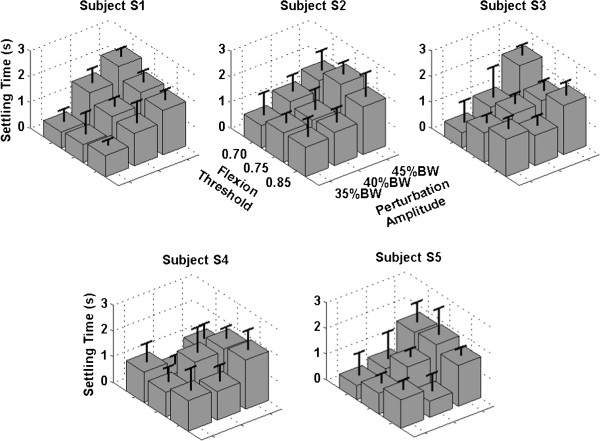
Methods: A feedback control system for maintaining seated balance under external perturbations was designed and tested in individuals with thoracic and cervical level spinal cord injuries. The control system relied on a signal related to the tilt of the trunk from the vertical position (which varied between 1.0 ≡ erect posture and 0.0 ≡ most forward flexed posture) derived from a sensor fixed to the sternum to activate the user's own hip and trunk extensor muscles via an implanted neuroprosthesis. A proportional-derivative controller modulated stimulation between trunk tilt values indicating deviation from the erect posture and maximum desired forward flexion. Tests were carried out with external perturbation forces set at 35%, 40% and 45% body-weight (BW) and maximal forward trunk tilt flexion thresholds set at 0.85, 0.75 and 0.70.
Results: Preliminary tests in a case series of five subjects show that the controller could maintain trunk stability in the sagittal plane for perturbations up to 45% of body weight and for flexion thresholds as low as 0.7. The mean settling time varied across subjects from 0.5(±0.4) and 2.0 (±1.1) seconds. Mean response time of the feedback control system varied from 393(±38) ms and 536(±84) ms across the cohort.
Conclusions: The results show the high potential for robust control of seated balance against nominal perturbations in individuals with spinal cord injury and indicates that trunk control with FNS is a promising intervention for individuals with SCI.
Figures



References
-
- Marsolais EB, Kobetic R. Implantation techniques and experience with percutaneous intramuscular electrodes in the lower extremities. J Rehabil Res Dev. 1986;23(3):1–8. - PubMed
-
- Triolo RJ, Kobetic R, Betz R. Standing and walking with FNS: technical and clinical challenges. In: Harris G, editor. Human motion analysis. New York NY: IEEE Press; 1996. pp. 318–350.
-
- Thrasher TA, Sin VW, Masani K, Vette AH, Craven BC, Popovic MR. Responses of the trunk to multidirectional perturbations during unsupported sitting. J Appl Biomech. 2010;26:332–340. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
