

High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study
- PMID: 25609052
- PMCID: PMC4301191
- DOI: 10.1136/bmj.g7873
High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study
Erratum in
-
High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study.BMJ. 2015 Feb 3;350:h626. doi: 10.1136/bmj.h626. BMJ. 2015. PMID: 25646958 Free PMC article. No abstract available.
-
High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study.BMJ. 2016 Sep 6;354:i4840. doi: 10.1136/bmj.i4840. BMJ. 2016. PMID: 27600543 Free PMC article. No abstract available.
Abstract
Objective: To evaluate the diagnosis of myocardial infarction using a high sensitivity troponin I assay and sex specific diagnostic thresholds in men and women with suspected acute coronary syndrome.
Design: Prospective cohort study.
Setting: Regional cardiac centre, United Kingdom.
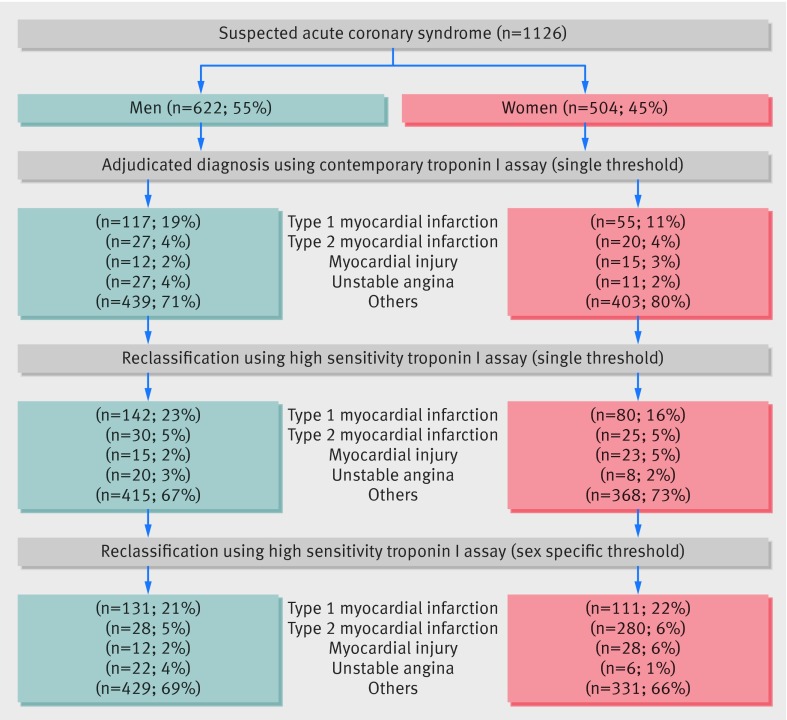
Participants: Consecutive patients with suspected acute coronary syndrome (n=1126, 46% women). Two cardiologists independently adjudicated the diagnosis of myocardial infarction by using a high sensitivity troponin I assay with sex specific diagnostic thresholds (men 34 ng/L, women 16 ng/L) and compared with current practice where a contemporary assay (50 ng/L, single threshold) was used to guide care.
Main outcome measure: Diagnosis of myocardial infarction.
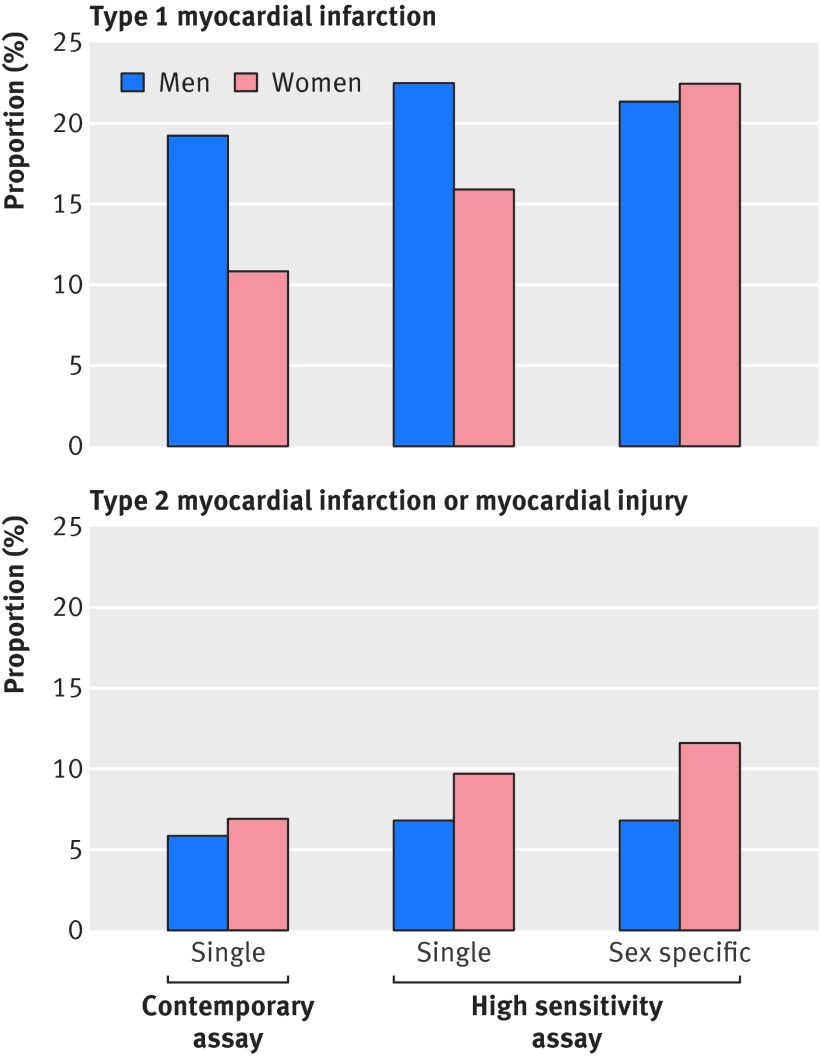
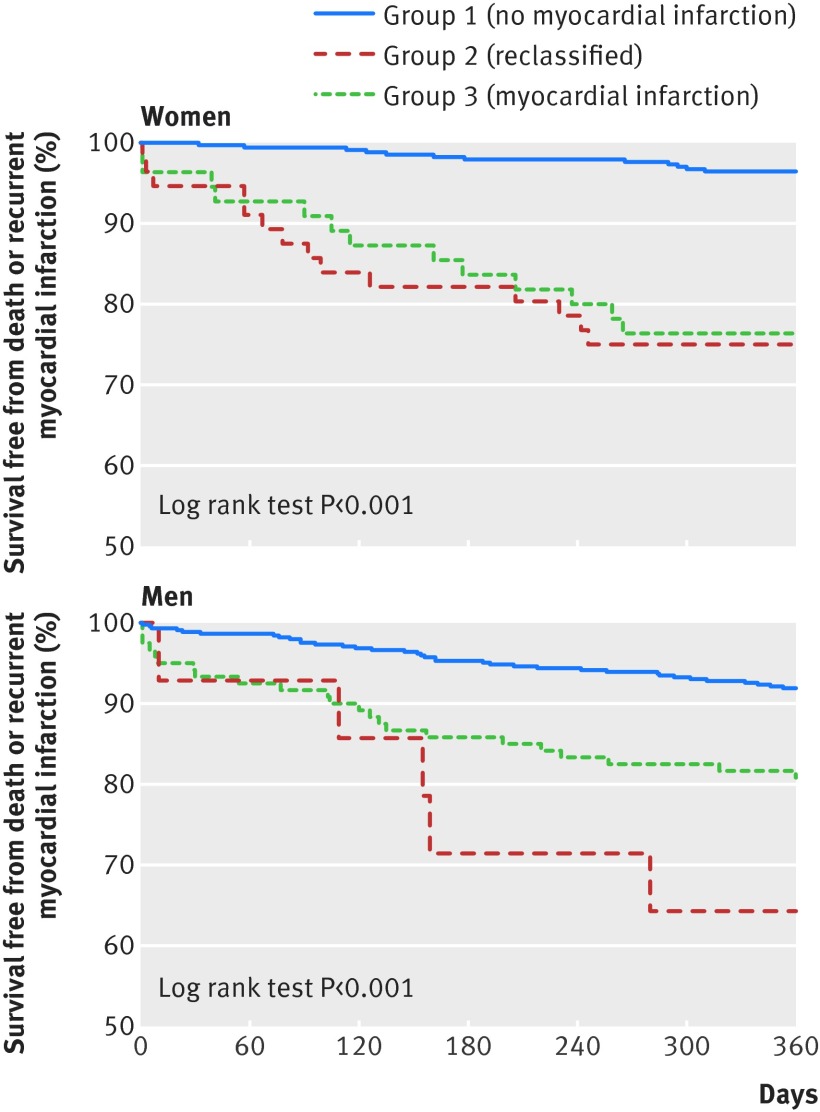
Results: The high sensitivity troponin I assay noticeably increased the diagnosis of myocardial infarction in women (from 11% to 22%; P<0.001) but had a minimal effect in men (from 19% to 21%, P=0.002). Women were less likely than men to be referred to a cardiologist or undergo coronary revascularisation (P<0.05 for both). At 12 months, women with undisclosed increases in troponin concentration (17-49 ng/L) and those with myocardial infarction (≥50 ng/L) had the highest rate of death or reinfarction compared with women without (≤16 ng/L) myocardial infarction (25%, 24%, and 4%, respectively; P<0.001).
Conclusions: Although having little effect in men, a high sensitivity troponin assay with sex specific diagnostic thresholds may double the diagnosis of myocardial infarction in women and identify those at high risk of reinfarction and death. Whether use of sex specific diagnostic thresholds will improve outcomes and tackle inequalities in the treatment of women with suspected acute coronary syndrome requires urgent attention.
© Shah et al 2015.
Conflict of interest statement
NLM and ASVS has acted as a consultant for Abbott Laboratories and Beckman-Coulter. FSA has acted as a consultant and received research funding from Siemens, Abbott Laboratories and Roche. All other authors have no conflicts of interest.
Figures
Comment in
-
Heart attack in women.Emerg Nurse. 2015 Feb;22(9):17. doi: 10.7748/en.22.9.17.s19. Emerg Nurse. 2015. PMID: 25659792 No abstract available.
-
Hochsensitiver Troponintest - Diagnose Infarkt: niedriger Schwellenwert umstritten.Dtsch Med Wochenschr. 2015 Mar;140(6):392. doi: 10.1055/s-0041-101005. Epub 2015 Mar 16. Dtsch Med Wochenschr. 2015. PMID: 25774725 German. No abstract available.
-
High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study.Ann Clin Biochem. 2015 Sep;52(Pt 5):622. Ann Clin Biochem. 2015. PMID: 26528515 No abstract available.
-
High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study.Ann Clin Biochem. 2015 Sep;52(5):622. doi: 10.1177/0004563215597105. Ann Clin Biochem. 2015. PMID: 28071101 No abstract available.
References
-
- Gan SC, Beaver SK, Houck PM, MacLehose RF, Lawson HW, Chan L. Treatment of acute myocardial infarction and 30-day mortality among women and men. N Engl J Med 2000;343:8-15. - PubMed
-
- Vaccarino V, Krumholz HM, Yarzebski J, Gore JM, Goldberg RJ. Sex differences in 2-year mortality after hospital discharge for myocardial infarction. Ann Intern Med 2001;134:173-81. - PubMed
-
- Anderson RD, Pepine CJ. Gender differences in the treatment for acute myocardial infarction: bias or biology? Circulation 2007;115:823-6. - PubMed
-
- Canto JG, Goldberg RJ, Hand MM, Bonow RO, Sopko G, Pepine CJ, et al. Symptom presentation of women with acute coronary syndromes: myth vs reality. Arch Intern Med 2007;167:2405-13. - PubMed
-
- Elsaesser A, Hamm CW. Acute coronary syndrome: the risk of being female. Circulation 2004;109:565-7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous