

Contributors to primary care guidelines: What are their professions and how many of them have conflicts of interest?
- PMID: 25609522
- PMCID: PMC4301766
Contributors to primary care guidelines: What are their professions and how many of them have conflicts of interest?
Abstract
Objective: To determine the professions of those who contribute to guidelines, guideline variables associated with differing contributor participation, and whether conflict of interest statements are provided in primary care guidelines.
Design: Retrospective analysis of the primary care guidelines from the Canadian Medical Association website. Two independent data extractors reviewed the guidelines and extracted relevant data.
Setting: Canada.
Main outcome measures: Sponsors of guidelines, jurisdiction (national or provincial) of guidelines, the professions of those who contribute to guidelines, and the reported conflict of interest statements within guidelines.
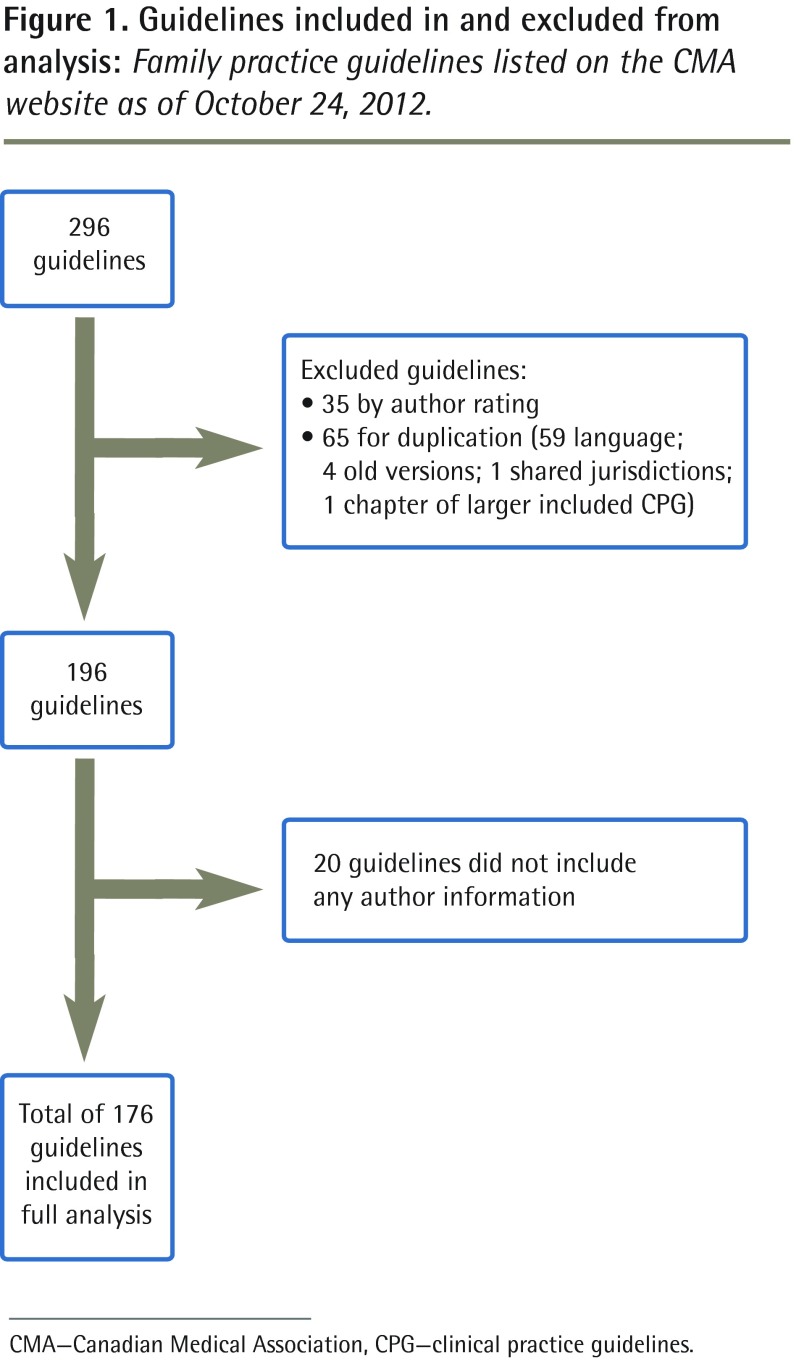
Results: Of the 296 guidelines in the family medicine section of the CMA Infobase, 65 were duplicates and 35 had limited relevance to family medicine. Twenty did not provide contributor information, leaving 176 guidelines for analysis. In total, there were 2495 contributors (authors and committee members): 1343 (53.8%) non-family physician specialists, 423 (17.0%) family physicians, 141 (5.7%) nurses, 75 (3.0%) pharmacists, 269 (10.8%) other clinicians, 203 (8.1%) nonclinician scientists, and 41 (1.6%) unknown professions. The proportion of contributors from the various professions differed significantly between provincial and national guidelines, as well as between industry-funded and non-industry-funded guidelines (both P < .001). For provincial guidelines, 30.8% of contributors were family physicians and 37.3% were other specialists compared with 13.9% and 57.4%, respectively, for national guidelines. Of industry-funded guidelines, 7.8% of contributors were family physicians and 68.6% were other specialists compared with 19.4% and 49.9%, respectively, for non-industry-funded guidelines. Conflicts of interest were not reported in 68.9% of guidelines. When reported, conflict of interest statements were present for 48.6% of non-family physician specialists, 30.0% of pharmacists, 27.7% of family physicians, and 10.0% or less of the remaining groups; differences were statistically significant (P < .001).
Conclusion: Non-family physician specialists outnumber all other health care providers combined and are more than 3 times more likely to contribute to primary care guidelines than family physicians are. Conflict of interest statements were provided in the minority of guidelines, and for guidelines in which conflict of interest statements were included, non-family physician specialists were most likely to report them. Guidelines targeted to primary care should have much more primary care and family medicine representation and include fewer contributors who have conflicts of interest.
Copyright© the College of Family Physicians of Canada.
Figures
References
-
- DeGuzman PB, Akosah KO, Simpson AG, Barbieri KE, Megginson GC, Goldberg RI, et al. Sub-optimal achievement of guideline-derived lipid goals in management of diabetes patients with atherosclerotic cardiovascular disease, despite high use of evidence-based therapies. Diab Vasc Dis Res. 2012;19(2):138–45. Epub 2012 Jan 10. - PubMed
-
- Lee DH, Vielemeyer O. Analysis of overall level of evidence behind Infectious Diseases Society of America practice guidelines. Arch Intern Med. 2011;171(1):18–22. - PubMed
-
- Tricoci P, Allen JM, Kramer JM, Califf RM, Smith SC., Jr Scientific evidence underlying the ACC/AHA clinical practice guidelines. JAMA. 2009;301(8):831–41. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources