

Sigmoid volvulus
- PMID: 25610145
- PMCID: PMC4261258
- DOI: 10.5152/eajm.2010.39
Sigmoid volvulus
Abstract
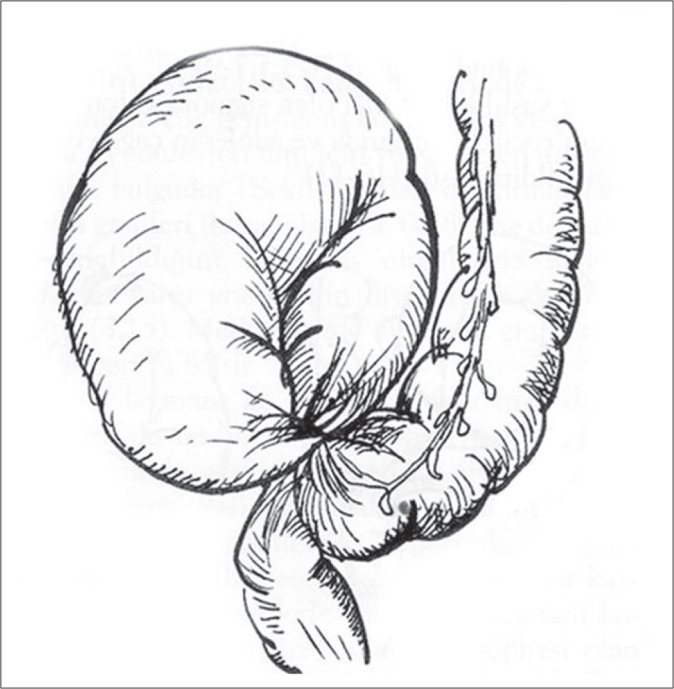
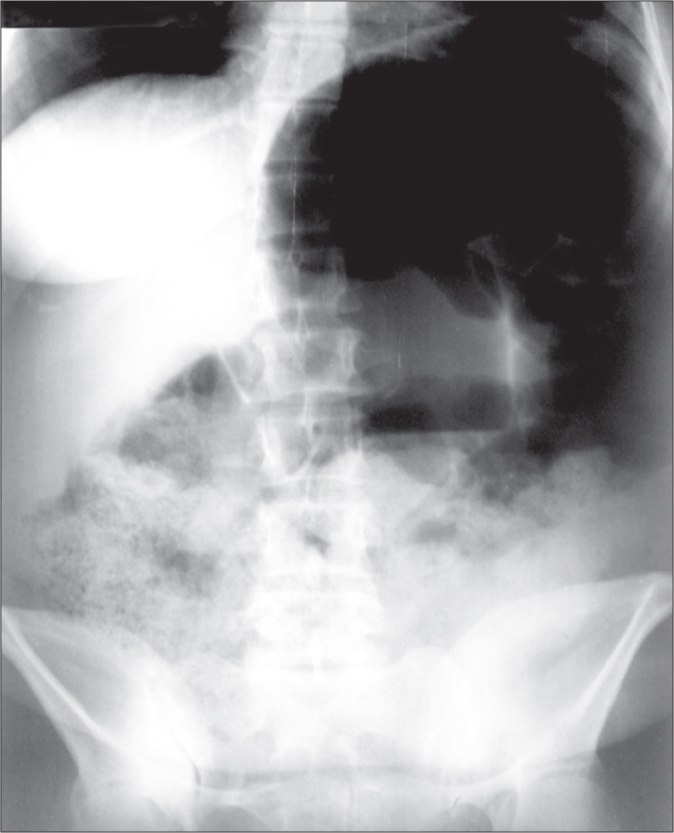
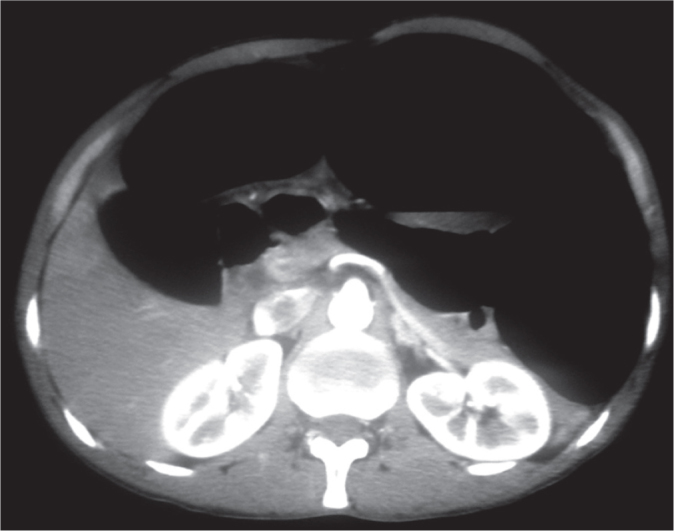
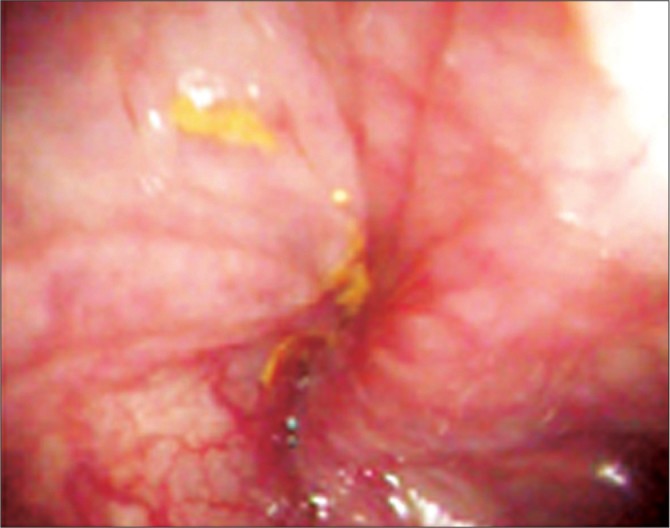
In sigmoid volvulus (SV), the sigmoid colon wraps around itself and its mesentery. SV accounts for 2% to 50% of all colonic obstructions and has an interesting geographic dispersion. SV generally affects adults, and it is more common in males. The etiology of SV is multifactorial and controversial; the main symptoms are abdominal pain, distention, and constipation, while the main signs are abdominal distention and tenderness. Routine laboratory findings are not pathognomonic: Plain abdominal X-ray radiographs show a dilated sigmoid colon and multiple small or large intestinal air-fluid levels, and abdominal CT and MRI demonstrate a whirled sigmoid mesentery. Flexible endoscopy shows a spiral sphincter-like twist of the mucosa. The diagnosis of SV is established by clinical, radiological, endoscopic, and sometimes operative findings. Although flexible endoscopic detorsion is advocated as the primary treatment choice, emergency surgery is required for patients who present with peritonitis, bowel gangrene, or perforation or for patients whose non-operative treatment is unsuccessful. Although emergency surgery includes various non-definitive or definitive procedures, resection with primary anastomosis is the most commonly recommended procedure. After a successful non-operative detorsion, elective sigmoid resection and anastomosis is recommended. The overall mortality is 10% to 50%, while the overall morbidity is 6% to 24%.
Sigmoid volvulus (SV), sigmoid kolonun kendisi ve mezenteri etrafında dönmesidir. SV, tüm kolonik tıkanıklıkların %2–50’sini oluşturur ve ilginç bir coğrafi dağılımı vardır. SV genellikle erişkinleri tutar ve erkeklerde daha sık görülür. SV’nin etiyolojisi çok faktörlü ve tartışmalıdır. Başlıca belirtiler karın ağrısı, şişkinlik ve gaz-gaita çıkaramama iken başlıca bulgular karında şişkinlik ve hassasiyettir. Rutin laboratuar bulguları hastalığa özgü değildir. Düz karın radyografileri genişlemiş bir sigmoid kolon ve çok sayıda ince ya da kalın barsak hava-sıvı seviyelerini gösterir. Karın CT veya MRI’ı dönmüş bir mezenteri ortaya koyar. Fleksibl endoskopi sfinkter benzeri spiral mukoza dönmesini gösterir. SV tanısı klinik, radyolojik, endoskopik ve bazen de operatif bulgulara dayanır. Her ne kadar fleksibl endoskopik detorsiyon başlangıç tedavi seçeneği olarak önerilirse de peritoniti, barsak gangreni veya perforasyonu olan veya nonoperatif tedavinin başarısız olduğu hastalarda acil cerrahi gerekir. Acil cerrahi değişik nondefinitif veya definitif işlemi kapsamakla birlikte, rezeksiyon ve primer anastomoz en çok önerilen işlemdir. Başarılı bir nonoperatif detorsiyon sonrası elektif sigmoid rezeksiyon ve anastomoz, iyi riskli hastalarda önerilir. Toplam mortalite %10–50 iken toplam morbidite %6–24’tür.
Keywords: Intestinal obstruction; Sigmoid colon; Volvulus.
Figures


Similar articles
-
Ileosigmoid knotting.Eurasian J Med. 2009 Aug;41(2):116-9. Eurasian J Med. 2009. PMID: 25610081 Free PMC article. Review.
-
Sigmoid volvulus in a teenager, successfully managed with endoscopic detorsion: An unusual case report and review of the literature.Int J Surg Case Rep. 2020;77:875-879. doi: 10.1016/j.ijscr.2020.11.152. Epub 2020 Dec 3. Int J Surg Case Rep. 2020. PMID: 33395915 Free PMC article.
-
Endoscopic detorsion of sigmoid volvulus in a young female: a case report.J Med Case Rep. 2024 Aug 13;18(1):378. doi: 10.1186/s13256-024-04578-0. J Med Case Rep. 2024. PMID: 39135144 Free PMC article.
-
The role of sigmoidoscopy in thediagnosis and treatment of sigmoid volvulus.Pak J Med Sci. 2016 Jan-Feb;32(1):244-8. doi: 10.12669/pjms.321.8410. Pak J Med Sci. 2016. PMID: 27022384 Free PMC article. Review.
-
Non-invasive treatment of sigmoid volvulus in a child. The role of the endoscopist.Ann Ital Chir. 2022;93:443-446. Ann Ital Chir. 2022. PMID: 36155995
Cited by
-
Sigmoid volvulus: a rare but unique complication of enteric fever.J Community Hosp Intern Med Perspect. 2020 Feb 10;10(1):45-49. doi: 10.1080/20009666.2020.1718480. eCollection 2020. J Community Hosp Intern Med Perspect. 2020. PMID: 32128058 Free PMC article.
-
Laceration of the transverse mesocolon in an old man with a habit of abdominal massage for constipation: a case report.Surg Case Rep. 2020 Jan 2;6(1):1. doi: 10.1186/s40792-019-0767-6. Surg Case Rep. 2020. PMID: 31898753 Free PMC article.
-
Factors precipitating volvulus formation in sigmoid volvulus.Ulus Travma Acil Cerrahi Derg. 2022 Mar;28(3):281-284. doi: 10.14744/tjtes.2020.03762. Ulus Travma Acil Cerrahi Derg. 2022. PMID: 35485550 Free PMC article.
-
Laparoscopic Sigmoid Colectomy with Natural Orifice Specimen Extraction in Sigmoid Volvulus.Eurasian J Med. 2024 May 2;56(2):142-5. doi: 10.5152/eurasianjmed.2024.24420. Online ahead of print. Eurasian J Med. 2024. PMID: 38798007 Free PMC article.
-
Endoscopic Decompression of Recurrent Sigmoid Volvulus in Pregnancy.J Investig Med High Impact Case Rep. 2020 Jan-Dec;8:2324709620975939. doi: 10.1177/2324709620975939. J Investig Med High Impact Case Rep. 2020. PMID: 33238755 Free PMC article.
References
-
- Raveenthiran R, Madiba TE, Atamanalp SS, De U. Volvulus of the sigmoid colon. Colorectal Dis. 2010;12:1–17. - PubMed
-
- Atamanalp SS, Yildirgan MI, Basoglu M, Kantarci M, Yilmaz I. Sigmoid colon volvulus in children: review of 19 cases. Pediatr Surg Int. 2004;20:492–5. - PubMed
-
- Lal SK, Morgenstern R, Vinjirayer EP, Matin A. Sigmoid volvulus an update. Gastrointest Endoscopy Clin N Am. 2006;16:175–87. - PubMed
-
- Madiba TE, Thomson SR, Corr P. Volvulus of the sigmoid colon. Gastroenterol Forum. 1997;8:28–33.
Publication types
LinkOut - more resources
Full Text Sources