

Comparison of two different doses of intrathecal levobupivacaine for transurethral endoscopic surgery
- PMID: 25610173
- PMCID: PMC4261346
- DOI: 10.5152/eajm.2011.23
Comparison of two different doses of intrathecal levobupivacaine for transurethral endoscopic surgery
Abstract
Objective: To evaluate the effects of two different spinal isobaric levobupivacaine doses on spinal anesthesia characteristics and to find the minimum effective dose for surgery in patients undergoing transurethral resection (TUR) surgery.
Materials and methods: Fifty male patients undergoing TUR surgery were included in the study and were randomized into two equal groups: Group LB10 (n=25): 10 mg 0.5% isobaric levobupivacaine (2 ml) and Group LB15 (n=25): 15 mg 0.75% isobaric levobupivacaine (2 ml). Spinal anesthesia was administered via a 25G Quincke spinal needle through the L3-4 intervertebral space. Sensorial block levels were evaluated using the 'pin-prick test', and motor block levels were evaluated using the 'Bromage scale'. The sensorial and motor block characteristics of patients during intraoperative and postoperative periods and recovery time from spinal anesthesia were evaluated.
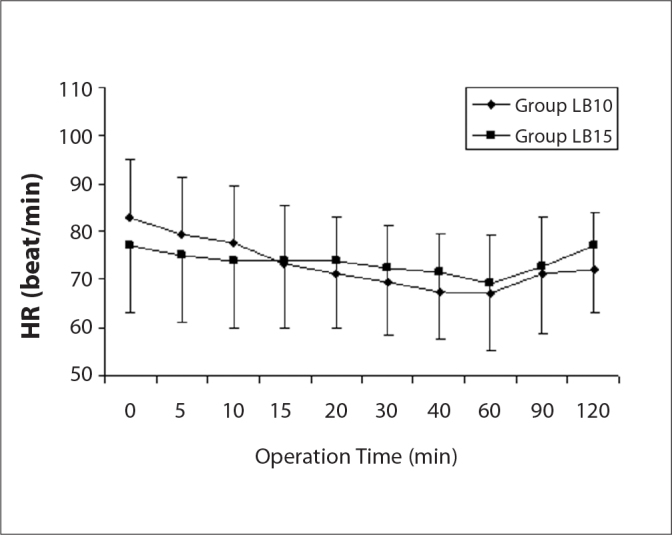
Results: In three cases in the Group LB10, sensorial block did not reach the T10 level. Complete motor block (Bromage=3) did not occur in eight cases in the Group LB10 and in five cases in the Group LB15. The highest sensorial dermatomal level detected was higher in Group LB15. In Group LB15, sensorial block initial time and the time of complete motor block occurrence were significantly shorter than Group LB10. Hypotension was observed in one case in Group LB15. No significant difference between groups was detected in two segments of regression times: the time to S2 regression and complete sensorial block regression time. Complete motor block regression time was significantly longer in Group LB15 than in Group LB10 (p<0.01).
Conclusion: Our findings showed that the minimum effective spinal isobaric levobupivacaine dose was 10 mg for TUR surgery.
Amaç: Spinal anestezi özellikleri iki farklı spinal izobarik levobupivakain dozlarının etkilerini değerlendirmek ve transüretral rezeksiyon (TUR) ameliyatı geçiren hastalarda cerrahi için etkili en düşük dozu bulmak.
Gereç ve yöntem: TUR ameliyatı Elli erkek hasta çalışmaya alındı ve iki eşit gruba ayrıldı: Grup LB10 (n=25): 10mg %0.5 izobarik levobupivakain (2 ml) ve Grup LB15 (n=25): 15 mg %0.75 izobarik levobupivakain (2 ml). Spinal anestezi L3–4 intervertebral uzayda bir 25G Quincke spinal iğne ile uygulandı. Duyusal blok seviyeleri ‘pin-prick testi’ ile değerlendirildi ve motor blok seviyeleri ‘Bromage ölçeği’ ile değerlendirildi. Spinal anestezi ile intraoperatif ve postoperatif dönem ve iyileşme süresi boyunca hastaların duyusal ve motor blok özellikleri değerlendirildi.
Bulgular: Grup LB10 üç durumlarda, duyusal blok seviyesi T10 ulaşmadı. Komple motor blok (Bromage=3) Grup LB10 ve Grup LB15 beş olguda sekiz olguda görülmedi. Tespit edilen en yüksek duyusal dermatomal Düzeyli Grup LB15 daha yüksekti. Grup LB15 olarak, duyusal blok başlangıç zamanı ve tam motor blok oluşma süresi Grup LB10 anlamlı olarak kısa bulundu. Hipotansiyon Grup LB15 bir durum gözlenmiştir. S2 regresyon ve tam duyusal blok gerileme zaman zaman: Gruplar arasında anlamlı bir fark regresyon kez iki segment saptandı. Komple motor blok gerileme zamanı Grup LB10 (p<0.01) daha Grubu LB15 anlamlı olarak daha uzundu.
Sonuç: Bu bulgular en az etkili spinal izobarik levobupivakain doz TUR ameliyatı için 10 mg olduğunu gösterdi.
Keywords: Levobupivacaine; Spinal anesthesia; Transurethral surgery.
Figures



Similar articles
-
ED50 and ED95 of intrathecal isobaric levobupivacaine coadministered with fentanyl for transurethral resections: randomized, double-blind trial.Drug Res (Stuttg). 2015 Jan;65(1):24-9. doi: 10.1055/s-0034-1370940. Epub 2014 Mar 25. Drug Res (Stuttg). 2015. PMID: 24668575 Clinical Trial.
-
A randomized clinical study comparing spinal anesthesia with isobaric levobupivacaine with fentanyl and hyperbaric bupivacaine with fentanyl in elective cesarean sections.Anesth Essays Res. 2015 Jan-Apr;9(1):57-62. doi: 10.4103/0259-1162.150169. Anesth Essays Res. 2015. PMID: 25886422 Free PMC article.
-
Comparison of intrathecal hyperbaric and isobaric levobupivacaine in urological surgery.Minerva Anestesiol. 2010 Jan;76(1):24-8. Epub 2009 Nov 24. Minerva Anestesiol. 2010. PMID: 20125070 Clinical Trial.
-
Comparison of levobupivacaine alone and in combination with fentanyl and sufentanil in patients undergoing transurethral resection of the prostate.J Res Med Sci. 2013 May;18(5):378-82. J Res Med Sci. 2013. PMID: 24174940 Free PMC article.
-
The comparison of levobupivacaine in continuous or single dose spinal anesthesia for transurethral resection of prostate surgery.Braz J Anesthesiol. 2014 Mar-Apr;64(2):89-97. doi: 10.1016/j.bjane.2013.03.007. Epub 2013 Oct 11. Braz J Anesthesiol. 2014. PMID: 24794450
Cited by
-
Comparison of Levobupivacaine and Levobupivacaine with Dexmedetomidine in Infraumbilical Surgeries Under Spinal Anesthesia.Anesth Essays Res. 2018 Jan-Mar;12(1):251-255. doi: 10.4103/aer.AER_227_17. Anesth Essays Res. 2018. PMID: 29628591 Free PMC article.
-
Comparison of levobupivacaine and levobupivacaine with fentanyl in infraumbilical surgeries under spinal anaesthesia.Anesth Essays Res. 2015 May-Aug;9(2):178-84. doi: 10.4103/0259-1162.152148. Anesth Essays Res. 2015. PMID: 26417124 Free PMC article.
References
-
- Lee YY, Muchhal K, Chan CK. Levobupivacaine versus racemic bupivacaine in spinal anesthesia for urological surgery. Anaesth Intensive Care. 2003;31:637–41. - PubMed
-
- Vanna O, Chumsang L, Thongmee S. Levobupivakain and bupivakain in spinal anesthesia for transurethral endoscopic surgery. J Med Assoc Thai. 2006;8:1333–9. - PubMed
-
- Cuvas O, Er AE, Ongen E, Basar H. Spinal anestesia for transuretral resection operations: bupivakain versus levobupivakain. Minerva Anestesiol. 2008;74:697–701. - PubMed
-
- Sen H, Purtuloglu T, Sızlan A, Yanarates O, et al. Comparison of intrathecal hyperbaric and isobaric levobupivacaine in urological surgery. Minerva Anestesiol. 2010;76:24–8. - PubMed
-
- Danelli G, Baciarello M, Di Cianni S, et al. Effects of baricity of 0.5% or 0.75% levobupivakain on the onset time of spinal anesthesia: a randomized trial. Can J Anaesth. 2008;55:501–6. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials