

Combining targeted therapy and immune checkpoint inhibitors in the treatment of metastatic melanoma
- PMID: 25610709
- PMCID: PMC4296084
- DOI: 10.7497/j.issn.2095-3941.2014.04.002
Combining targeted therapy and immune checkpoint inhibitors in the treatment of metastatic melanoma
Abstract
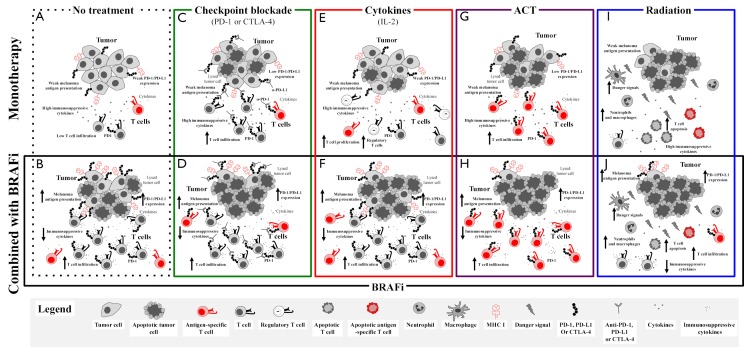
Melanoma is the deadliest form of skin cancer and has an incidence that is rising faster than any other solid tumor. Metastatic melanoma treatment has considerably progressed in the past five years with the introduction of targeted therapy (BRAF and MEK inhibitors) and immune checkpoint blockade (anti-CTLA4, anti-PD-1, and anti-PD-L1). However, each treatment modality has limitations. Treatment with targeted therapy has been associated with a high response rate, but with short-term responses. Conversely, treatment with immune checkpoint blockade has a lower response rate, but with long-term responses. Targeted therapy affects antitumor immunity, and synergy may exist when targeted therapy is combined with immunotherapy. This article presents a brief review of the rationale and evidence for the potential synergy between targeted therapy and immune checkpoint blockade. Challenges and directions for future studies are also proposed.
Keywords: BRAF inhibition; Melanoma; checkpoint blockade; immunotherapy.
Conflict of interest statement
Jennifer A. Wargo has honoraria from the speakers’ bureau of DAVA Oncology and is an advisory board member for Glaxo Smith Kline, Roche/Genentech, and Amgen. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A.Cancer statistics, 2014. CA Cancer J Clin 2014;64:9-29. - PubMed
-
- Little EG, Eide MJ. Update on the current state of melanoma incidence. Dermatol Clin 2012;30:355-361. - PubMed
-
- Beddingfield FC, 3rd. The melanoma epidemic: res ipsa loquitur. Oncologist 2003;8:459-465. - PubMed
-
- Costanza ME, Nathanson L, Costello WG, Wolter J, Brunk SF, Colsky J, et al. Results of a randomized study comparing DTIC with TIC mustard in malignant melanoma. Cancer 1976;37:1654-1659. - PubMed
-
- Patel PM, Suciu S, Mortier L, Kruit WH, Robert C, Schadendorf D, et al. Extended schedule, escalated dose temozolomide versus dacarbazine in stage IV melanoma: final results of a randomised phase III study (EORTC 18032). Eur J Cancer 2011;47:1476-1483. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous