

Heart failure with preserved ejection fraction
- PMID: 25610841
- PMCID: PMC4239812
- DOI: 10.5339/gcsp.2012.10
Heart failure with preserved ejection fraction
Abstract
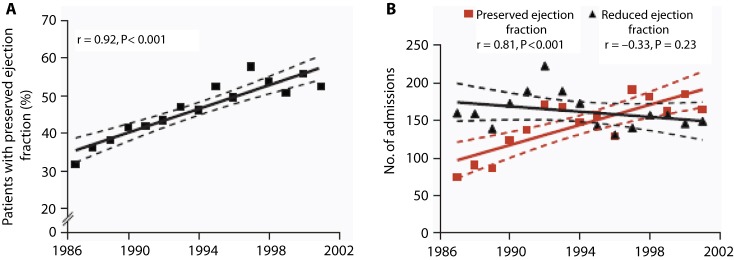
Heart failure with preserved ejection fraction (HFpEF) has recently emerged as a major cause of cardiovascular morbidity and mortality. Contrary to initial beliefs, HFpEF is now known to be as common as heart failure with reduced ejection fraction (HFrEF) and carries an unacceptably high mortality rate. With a prevalence that has been steadily rising over the past two decades, it is very likely that HFpEF will represent the dominant heart failure phenotype over the coming few years. The scarcity of trials in this semi-discrete form of heart failure and lack of unified enrolment criteria in the studies conducted to date might have contributed to the current absence of specific therapies. Understanding the epidemiological, pathophysiological and molecular differences (and similarities) between these two forms of heart failure is cornerstone to the development of targeted therapies. Carefully designed studies that adhere to unified diagnostic criteria with the recruitment of appropriate controls and adoption of practical end-points are urgently needed to help identify effective treatment strategies.
Keywords: diastolic heart failure; heart failure; heart failure with preserved ejection fraction.
Figures
References
-
- Bhatia RS, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. The New England Journal of Medicine. 2006;355:260–269. - PubMed
-
- Tribouilloy C, et al. Prognosis of heart failure with preserved ejection fraction: a 5 year prospective population-based study. European Heart Journal. 2008;29:339–347. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. Journal of the American College of Cardiology. 2004;43:317–327. - PubMed
-
- Redfield MM. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. Heart Failure. 2006:251–259. - PubMed
-
- Paulus WJ, van Ballegoij JJM. Treatment of heart failure with normal ejection fraction: an inconvenient truth! Journal of the American College of Cardiology. 2010;55:526–537. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous