

Characterizing the epidemiology of postoperative transfusion-related acute lung injury
- PMID: 25611652
- PMCID: PMC4844077
- DOI: 10.1097/ALN.0000000000000514
Characterizing the epidemiology of postoperative transfusion-related acute lung injury
Abstract
Background: Transfusion-related acute lung injury (TRALI) is the leading cause of transfusion-related death in the United States; however, it remains poorly characterized in surgical populations. To better inform perioperative transfusion practice, and to help mitigate perioperative TRALI, the authors aimed to better define its epidemiology before and after TRALI mitigation strategies were introduced.
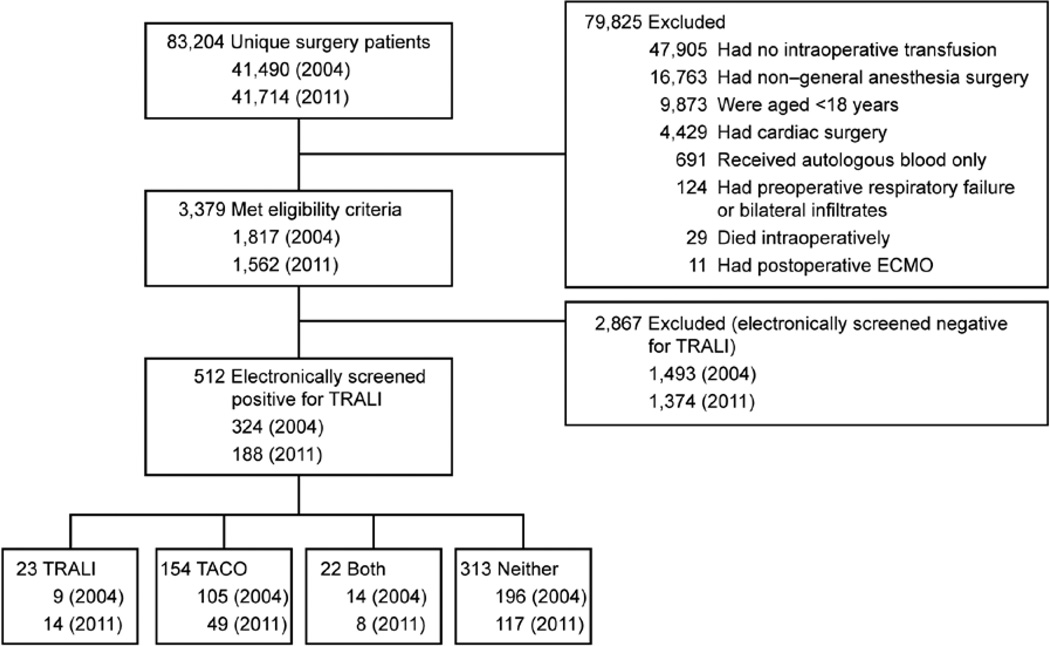
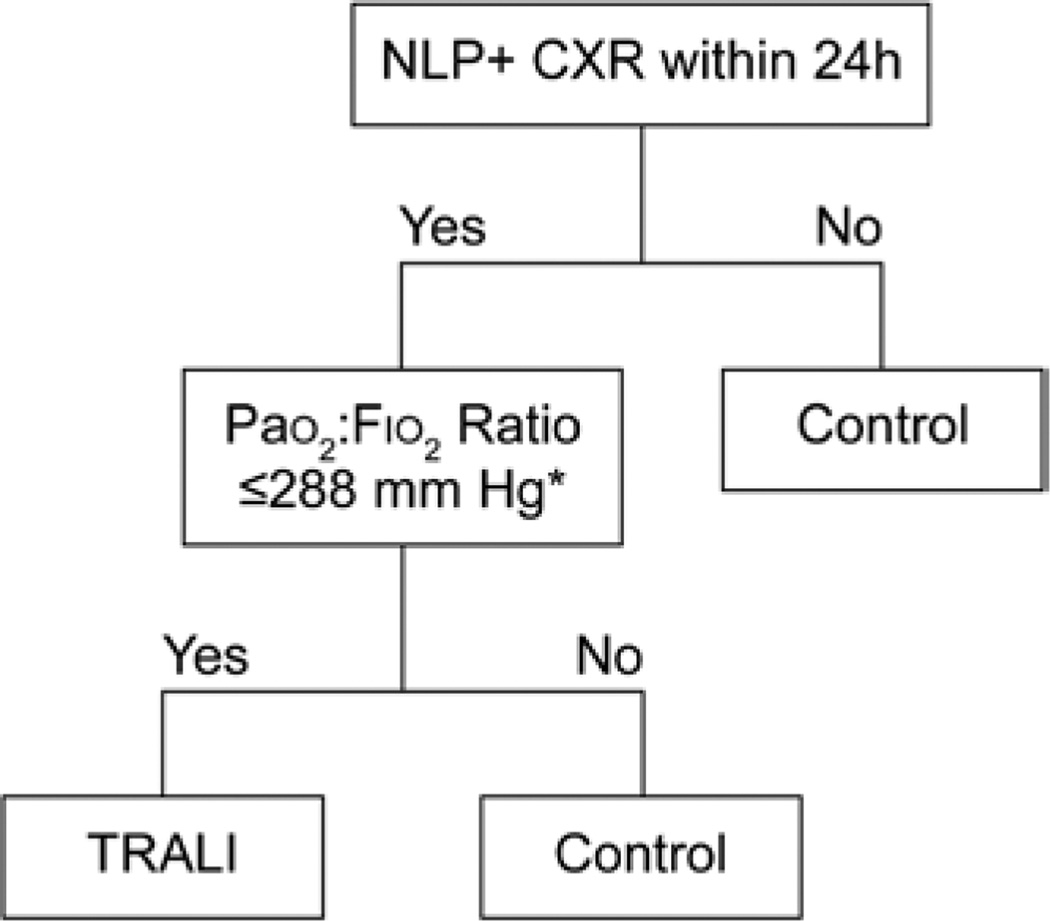
Methods: This retrospective cohort study examined outcomes of adult patients undergoing noncardiac surgery with general anesthesia who received intraoperative transfusions during 2004 (n = 1,817) and 2011 (n = 1,562). The demographics and clinical characteristics of transfusion recipients, blood transfusion descriptors, and combined TRALI/possible TRALI incidence rates were evaluated. Univariate analyses were used to compare associations between patient characteristics, transfusion details, and TRALI mitigation strategies with TRALI/possible TRALI incidence rates in a before-and-after study design.
Results: The incidence of TRALI/possible TRALI was 1.3% (23 of 1,613) in 2004 versus 1.4% (22 of 1,562) in 2011 (P = 0.72), with comparable overall rates in males versus females (1.4% [23 of 1,613] vs. 1.2% [22 of 1,766]) (P = 0.65). Overall, thoracic (3.0% [4 of 133]), vascular (2.7% [10 of 375]), and transplant surgeries (2.2% [4 of 178]) carried the highest rates of TRALI/possible TRALI. Obstetric and gynecologic surgical patients had no TRALI episodes. TRALI/possible TRALI incidence increased with larger volumes of blood product transfused (P < 0.001).
Conclusions: Perioperative TRALI/possible TRALI is more common than previously reported and its risk increases with greater volumes of blood component therapies. No significant reduction in the combined incidence of TRALI/possible TRALI occurred between 2004 and 2011, despite the introduction of TRALI mitigation strategies. Future efforts to identify specific risk factors for TRALI/possible TRALI in surgical populations may reduce the burden of this life-threatening complication.
Figures
Comment in
-
Revealing the real risks of perioperative transfusion: rise of the machines!Anesthesiology. 2015 Jan;122(1):1-2. doi: 10.1097/ALN.0000000000000515. Anesthesiology. 2015. PMID: 25611649 Free PMC article. No abstract available.
-
Transfusion-related Acute Lung Injury: More Questions Than Answers?Anesthesiology. 2015 Aug;123(2):488-9. doi: 10.1097/ALN.0000000000000733. Anesthesiology. 2015. PMID: 26196883 No abstract available.
References
-
- Fatalities Reported to FDA Following Blood Collection and Transfusion: Annual summary for fiscal year 2013: 2013 US Department of Health and Human Services. Rockville (MD: US Food and Drug Administration;
-
- Kopko PM, Marshall CS, MacKenzie MR, Holland PV, Popovsky MA. Transfusion-related acute lung injury: Report of a clinical look-back investigation. JAMA. 2002;287:1968–1971. - PubMed
-
- Gajic O, Rana R, Winters JL, Yilmaz M, Mendez JL, Rickman OB, O’Byrne MM, Evenson LK, Malinchoc M, DeGoey SR, Afessa B, Hubmayr RD, Moore SB. Transfusion-related acute lung injury in the critically ill: Prospective nested case-control study. Am J Respir Crit Care Med. 2007;176:886–891. - PMC - PubMed
-
- Popovsky MA, Moore SB. Diagnostic and pathogenetic considerations in transfusion-related acute lung injury. Transfusion. 1985;25:573–577. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
