

Treatment-related biomarkers in pulmonary hypertension
- PMID: 25611885
- PMCID: PMC4491132
- DOI: 10.1165/rcmb.2014-0438TR
Treatment-related biomarkers in pulmonary hypertension
Abstract
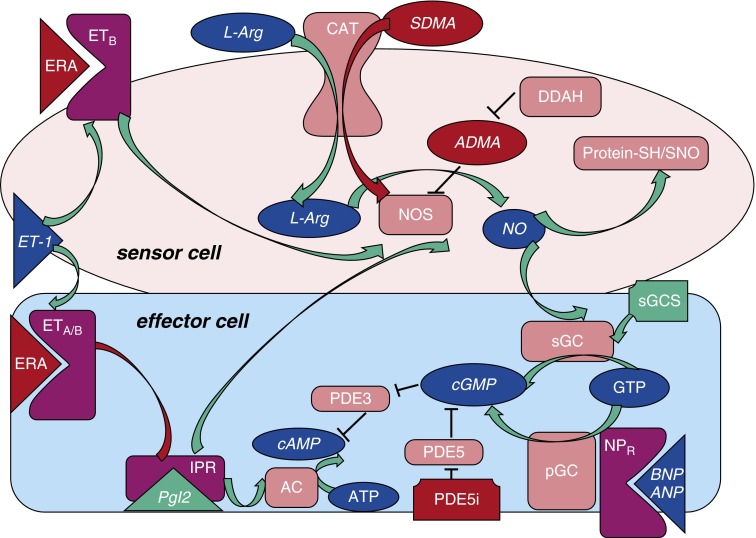
Significant advances in the treatment of pulmonary arterial hypertension (PAH) over the last two decades have led to the introduction of multiple classes of oral therapy, but the disease remains devastating for many patients. Disease progression, in spite of oral monotherapy, is a major problem, and alternative therapy, such as infusion of prostacyclins, is cumbersome and carries considerable potential morbidity. Use of combination oral therapy, including drugs from both the endothelin receptor antagonist and phosphodiesterase-5 inhibitor classes, has increased, and there is some evidence to support this approach. Given the multiple options now available in pulmonary hypertension (PH) therapy, biomarkers to guide treatment decisions could be helpful. Here, we review the evidence for and against the clinical use of molecular biomarkers relevant to PH pathogenesis, emphasizing assayable markers that may also inform more rational selection of agents that influence pathways targeted by treatment. We emphasize the interactive nature of changes in mediators and messengers, such as endothelin-1, prostacyclin, brain natriuretic peptide (which has demonstrated biomarker utility), nitric oxide derivatives, and cyclic guanosine monophosphate, which play important roles in processes central to progression of PAH, such as vascular remodeling, vasoconstriction, and maladaptive right ventricular changes, and are relevant to its therapy. Accordingly, we propose that the identification and use of a molecular biomarker panel that assays these molecules in parallel and serially might, if validated, better inform unique patient phenotypes, prognosis, and the rational selection and titration of combination oral and other therapy in individual patients with PH/PAH.
Keywords: biomarker; endothelin; nitric oxide; right ventricle.
Figures
References
-
- Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF, Chabot F, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–1030. - PubMed
-
- Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JS, Howard LS, Pepke-Zaba J, Sheares KK, Corris PA, et al. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension: results from the pulmonary hypertension registry of the United Kingdom and Ireland. Am J Respir Crit Care Med. 2012;186:790–796. - PubMed
-
- Dweik RA, Rounds S, Erzurum SC, Archer S, Fagan K, Hassoun PM, Hill NS, Humbert M, Kawut SM, Krowka M, et al. ATS Committee on Pulmonary Hypertension Phenotypes. An official American Thoracic Society statement: pulmonary hypertension phenotypes. Am J Respir Crit Care Med. 2014;189:345–355. - PMC - PubMed
-
- Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med. 2004;351:1655–1665. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
