

Definitive radiotherapy for primary vaginal cancer: correlation between treatment patterns and recurrence rate
- PMID: 25614068
- PMCID: PMC4380060
- DOI: 10.1093/jrr/rru115
Definitive radiotherapy for primary vaginal cancer: correlation between treatment patterns and recurrence rate
Abstract
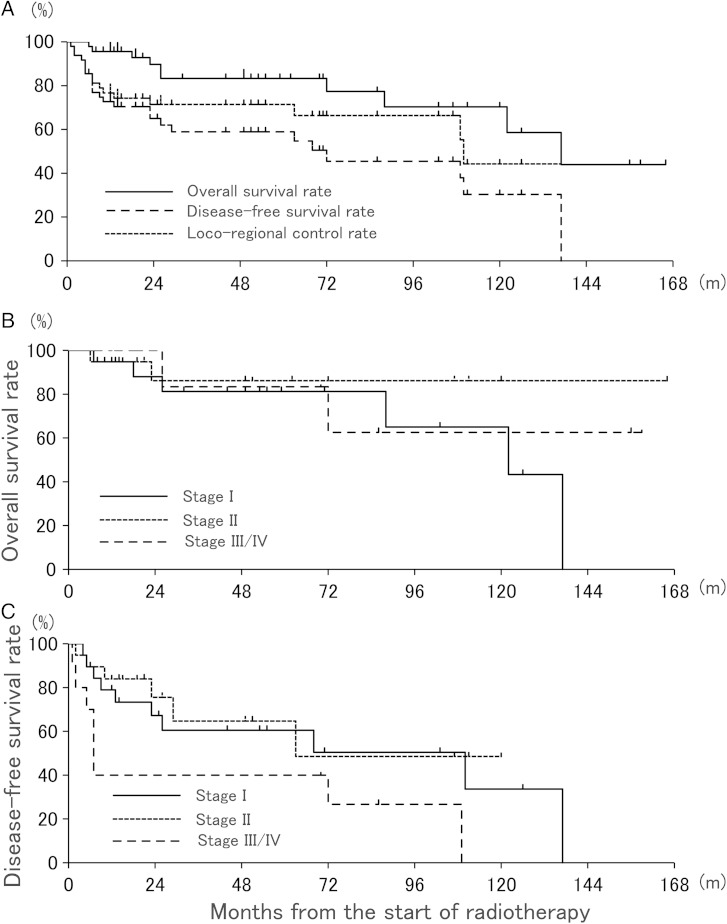
The purpose of this study was to determine the outcomes and optimal practice patterns of definitive radiotherapy for primary vaginal cancer. Between 1993 and 2012, 49 patients were treated with definitive radiotherapy for primary vaginal cancer in three hospitals. Of these, 15 patients (31%) had clinically positive regional lymph node metastasis. A total of 34 patients (70%) received external beam radiotherapy with high-dose-rate brachytherapy (interstitial or intracavitary), and 8 (16%) (with small superficial Stage I tumors) were treated with local radiotherapy. The median follow-up was 33 months (range: 1-169 months). The 3-year overall survival (OS), disease-free survival (DFS), and loco-regional control (LRC) rates were 83%, 59% and 71%, respectively. In multivariate analysis, the histological type (P = 0.044) was significant risk factors for LRC. In Federation of Gynecology and Obstetrics (FIGO) Stage I cases, 3 of 8 patients (38%) who did not undergo prophylactic lymph node irradiation had lymph node recurrence, compared with 2 of 12 patients (17%) who underwent prophylactic pelvic irradiation. For Stage III-IV tumors, the local recurrence rate was 50% and the lymph node recurrence rate was 40%. Patients with FIGO Stage I/II or clinical Stage N1 had a higher recurrence rate with treatment using a single modality compared with the recurrence rate using combined modalities. In conclusion, our treatment outcomes for vaginal cancer were acceptable, but external beam radiotherapy with brachytherapy (interstitial or intracavitary) was needed regardless of FIGO stage. Improvement of treatment outcomes in cases of FIGO Stage III or IV remains a significant challenge.
Keywords: high-dose-rate brachytherapy; prophylactic pelvic irradiation; radiotherapy; vaginal cancer.
© The Author 2015. Published by Oxford University Press on behalf of The Japan Radiation Research Society and Japanese Society for Radiation Oncology.
Figures
References
-
- Hacker NF, Eifel PJ, van der Velden J. Cancer of the vagina. Int J Gynaecol Obstet. 2012;119S2:S97–9. - PubMed
-
- Nonaka T, Nakayama Y, Mizoguchi N, et al. Definitive radiation therapy for invasive carcinoma of the vagina: impact of high-dose rate intracavitary brachytherapy. Int J Clin Oncol. 2013;18:314–20. - PubMed
-
- Mock U, Kucera H, Fellner C, et al. High-dose-rate (HDR) brachytherapy with or without external beam radiotherapy in the treatment of primary vaginal carcinoma: long-term results and side effects. Int J Radiat Oncol Biol Phys. 2003;56:950–7. - PubMed
-
- Nanavati PJ, Fanning J, Hilgers RD, et al. High-dose-rate brachytherapy in primary stage I and II vaginal cancer. Gynecol Oncol. 1993;51:67–71. - PubMed
-
- Kushner DM, Fleming PA, Kennedy AW, et al. High dose rate 192Ir afterloading brachytherapy for cancer of the vagina. Br J Radiol. 2003;76:719–725. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
