

CKD in elderly patients managed without dialysis: survival, symptoms, and quality of life
- PMID: 25614492
- PMCID: PMC4317735
- DOI: 10.2215/CJN.03330414
CKD in elderly patients managed without dialysis: survival, symptoms, and quality of life
Abstract
Background and objectives: Survival, symptom burden, and quality of life (QOL) are uncertain for elderly patients with advanced CKD managed without dialysis. We examined these outcomes in patients managed with renal supportive care without dialysis (RSC-NFD) and those planned for or commencing dialysis.
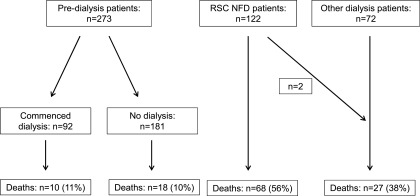
Design, setting, participants, & measurements: In this prospective observational study, symptoms were measured using the Memorial Symptom Assessment Scale and the Palliative care Outcomes Scale - Symptoms (renal) inventory and QOL was measured using the Short Form-36 survey. This study comprised 273 predialysis patients who had usual nephrology care and 122 nondialysis pathway patients who also attended a renal supportive care clinic adding the skills of a palliative medicine team. A further 72 patients commenced dialysis during this period without attending either clinic.
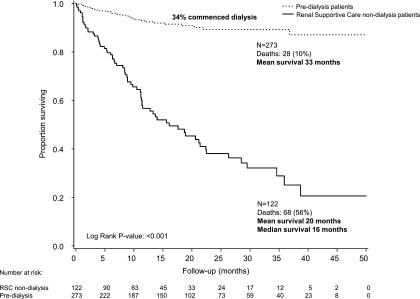
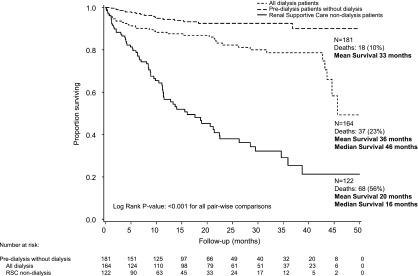
Results: Nondialysis patients were older than the predialysis group (82 versus 67 years; P<0.001) but had similar eGFR at the first clinic visit (16 ml/min per 1.73 m(2); P=0.92). Of the predialysis patients, 92 (34%) commenced dialysis. Compared with the RSC-NFD group, the death rate was lower in the predialysis group who did not require dialysis (hazard ratio, 0.23; 95% confidence interval, 0.12 to 0.41] and in those requiring dialysis (0.30; 0.13 to 0.67) but not in dialysis patients who had not attended the predialysis clinic (0.60; 0.35 to 1.03). Median survival in RSC-NFD patients was 16 (interquartile range, 9, 37) months and 32% survived >12 months after eGFR fell below 10 ml/min per 1.73 m(2). For the whole group, age, serum albumin, and eGFR <15 ml/min per 1.73 m(2) were associated with poorer survival. Of the nondialysis patients, 57% had stable or improved symptoms over 12 months and 58% had stable or improved QOL.
Conclusions: Elderly patients who choose not to have dialysis as part of shared decision making survive a median of 16 months and about one-third survive 12 months past a time when dialysis might have otherwise been indicated. Utilizing the skills of palliative medicine helps provide reasonable symptom control and QOL without dialysis.
Keywords: dialysis; elderly patients; palliative care; renal supportive care.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Four plus forty-four: hours to modify, theirs to enjoy.Clin J Am Soc Nephrol. 2015 Feb 6;10(2):169-71. doi: 10.2215/CJN.12681214. Epub 2015 Jan 22. Clin J Am Soc Nephrol. 2015. PMID: 25614491 Free PMC article. No abstract available.
References
-
- Swidler MA: Geriatric renal palliative care. J Gerontol A Biol Sci Med Sci 67: 1400–1409, 2012 - PubMed
-
- Australian and New Zealand Dialysis and Transplant Registry : ANZDATA 35th Annual Report, Adelaide, South Australia, ANZDATA, 2012
-
- US Renal Data System: Incidence, prevelance, patient characteristics, and treatment modalities, 2013. Available at: http://www.usrds.org/2013/pdf/v2_ch1_13.pdf. Accessed October 22, 2014
-
- UK Renal Registry: UK RRT Incidence in 2011: National and centre-specific analyses, 2011. Available at: http://www.renalreg.org/wp-content/uploads/2014/09/Chapter_1.pdf. Accessed October 22, 2014
-
- Brown MA, Crail SM, Masterson R, Foote C, Robins J, Katz I, Josland E, Brennan F, Stallworthy EJ, Brennan F, Siva B, Crail S, Brennan F, Siva B, Brennan F, Brown M, Miller C, Urban AK, Sajiv C, Stallworthy EJ, Glavish RN, May S, Langham R, Walker R, Fassett RG, Morton RL, Crail SM, Stewart C, Brennan F, Phipps L, Walker R, Healy H, Berquier I, Crail SM, Australian and New Zealand Society of Nephrology : ANZSN renal supportive care 2013: Opinion pieces [corrected]. Nephrology (Carlton) 18: 401–454, 2013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
