

Optimal doses of methotrexate combined with anti-TNF therapy to maintain clinical remission in inflammatory bowel disease
- PMID: 25616487
- PMCID: PMC4621545
- DOI: 10.1093/ecco-jcc/jjv027
Optimal doses of methotrexate combined with anti-TNF therapy to maintain clinical remission in inflammatory bowel disease
Abstract
Background and aims: Methotrexate (MTX) is sometimes used as part of combination therapy for the treatment of inflammatory bowel disease [IBD]; however, the optimal MTX dose for combination therapy has not been established. This study compared the efficacy of lower-dose and higher-dose MTX with anti tumor necrosis factor alpha (anti-TNF) therapy among IBD patients.
Methods: Retrospective chart review was performed of 88 IBD patients at our center between 2010 and 2013. Low-dose MTX was defined as ≤ 12.5mg/week and high-dose MTX as 15-25mg/week. Patients who met the criteria for clinical remission [Harvey-Bradshaw Index ≤ 4, Simple Clinical Colitis Activity Index ≤ 2] at baseline were followed for up to 42 months. Chart review occurred in 6-month intervals. The primary outcome was consecutive months in remission prior to relapse. Secondary outcomes included other indicators of worsening disease [endoscopic inflammation, steroid use, therapy escalation/addition, or surgery] and adverse events. Regression analysis and Kaplan-Meier survival analysis were completed.
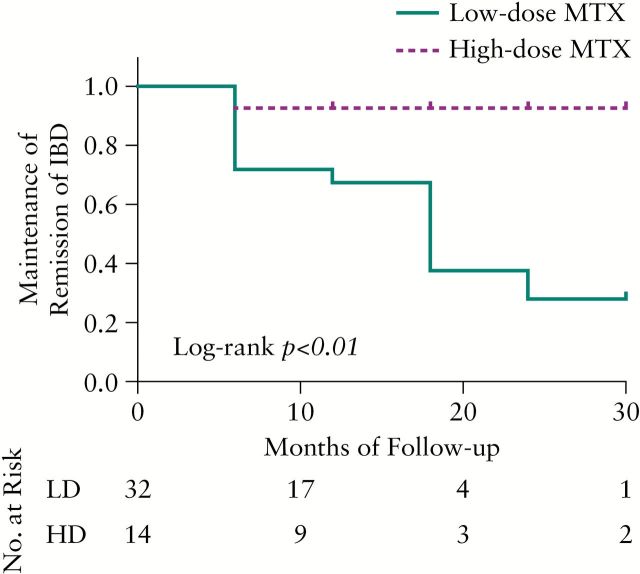
Results: We identified 73 [83%] dual-therapy patients, of whom 32 low-dose and 14 high-dose individuals achieved remission. When compared with high-dose patients, low-dose patients were more likely to relapse [log-rank test, p < 0.01]. Secondary indicators of worsening disease occurred during 34.4% of low-dose review periods and 31.4% of high-dose review periods [p = 0.67]; 3/52 [6%] low-dose patients and 3/21 [14%] high-dose patients [p = 0.34] discontinued MTX therapy due to adverse events.
Conclusions: When combined with anti-TNF therapy, MTX at doses of >12.5mg/week was more effective at maintaining clinical remission than lower doses. These findings will guide management of combination therapy in IBD patients.
Keywords: Methotrexate; adalimumab; anti-TNF therapy; certolizumab-pegol; combination therapy; inflammatory bowel disease; infliximab; maintenance of remission.
Copyright © 2015 European Crohn’s and Colitis Organisation (ECCO). Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Lahiff C, Kane S, Moss AC. Drug development in inflammatory bowel disease: the role of the FDA. Inflamm Bowel Dis 2011;17:2585–93. - PubMed
-
- Farber S, Diamond LK. Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4-aminopteroyl-glutamic acid. N Engl J Med 1948;238:787–93. - PubMed
-
- Saag KG, Yazdany J, Alexander C, et al. Defining quality of care in rheumatology: the American College of Rheumatology white paper on quality measurement. Arthritis Care Res [Hoboken] 2011;63:2–9. - PubMed
-
- Lipsky PE, van der Heijde DM, St Clair EW, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group. N Engl J Med 2000;343:1594–602. - PubMed
-
- Breedveld FC, Weisman MH, Kavanaugh AF, et al. The PREMIER study: A multicenter, randomized, double-blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis Rheum 2006;54:26–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
