

A novel therapy to attenuate acute kidney injury and ischemic allograft damage after allogenic kidney transplantation in mice
- PMID: 25617900
- PMCID: PMC4305280
- DOI: 10.1371/journal.pone.0115709
A novel therapy to attenuate acute kidney injury and ischemic allograft damage after allogenic kidney transplantation in mice
Abstract
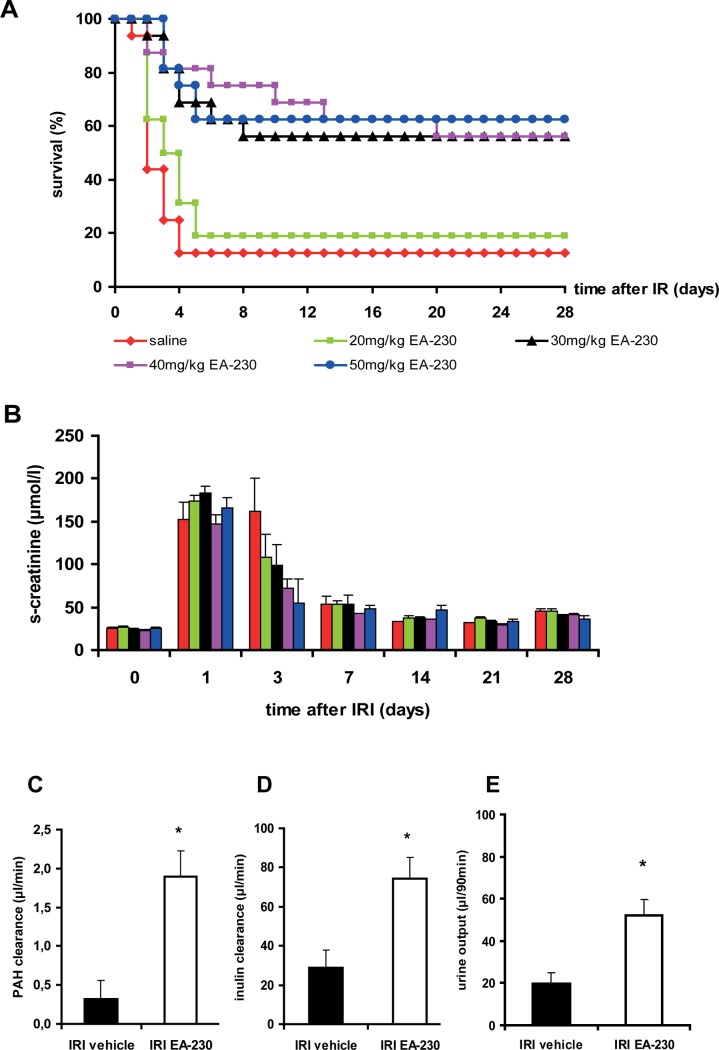
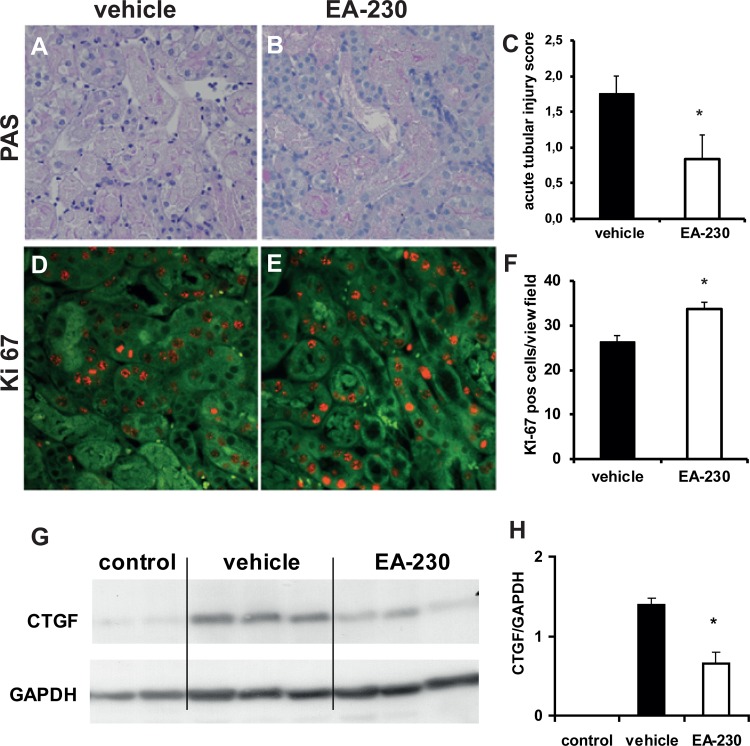
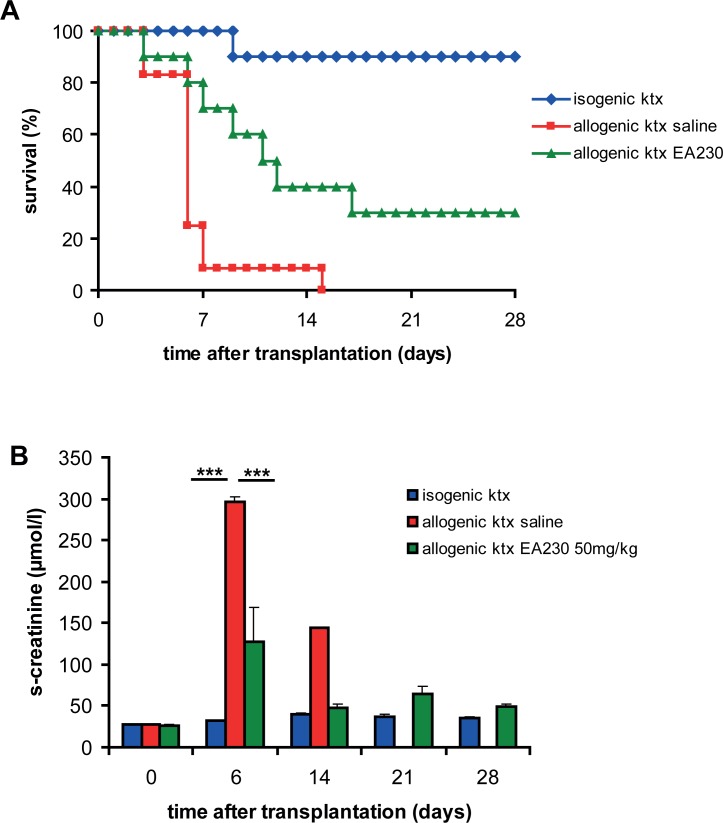
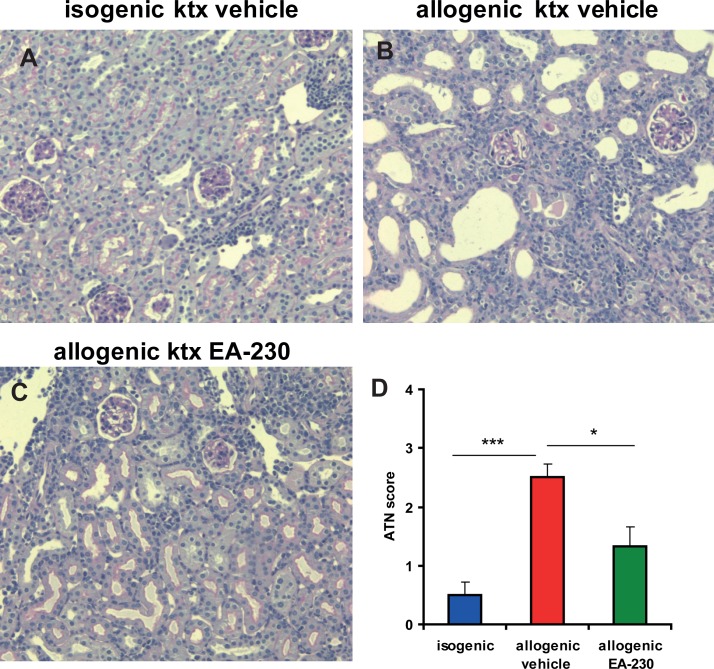
Ischemia followed by reperfusion contributes to the initial damage to allografts after kidney transplantation (ktx). In this study we tested the hypothesis that a tetrapeptide EA-230 (AQGV), might improve survival and attenuate loss of kidney function in a mouse model of renal ischemia/reperfusion injury (IRI) and ischemia-induced delayed graft function after allogenic kidney transplantation. IRI was induced in male C57Bl/6N mice by transient bilateral renal pedicle clamping for 35 min. Treatment with EA-230 (20-50mg/kg twice daily i.p. for four consecutive days) was initiated 24 hours after IRI when acute kidney injury (AKI) was already established. The treatment resulted in markedly improved survival in a dose dependent manner. Acute tubular injury two days after IRI was diminished and tubular epithelial cell proliferation was significantly enhanced by EA-230 treatment. Furthermore, CTGF up-regulation, a marker of post-ischemic fibrosis, at four weeks after IRI was significantly less in EA-230 treated renal tissue. To learn more about these effects, we measured renal blood flow (RBF) and glomerular filtration rate (GFR) at 28 hours after IRI. EA-230 improved both GFR and RBF significantly. Next, EA-230 treatment was tested in a model of ischemia-induced delayed graft function after allogenic kidney transplantation. The recipients were treated with EA-230 (50 mg/kg) twice daily i.p. which improved renal function and allograft survival by attenuating ischemic allograft damage. In conclusion, EA-230 is a novel and promising therapeutic agent for treating acute kidney injury and preventing IRI-induced post-transplant ischemic allograft injury. Its beneficial effect is associated with improved renal perfusion after IRI and enhanced regeneration of tubular epithelial cells.
Conflict of interest statement
Figures
Similar articles
-
Renal PKC-ε deficiency attenuates acute kidney injury and ischemic allograft injury via TNF-α-dependent inhibition of apoptosis and inflammation.Am J Physiol Renal Physiol. 2014 Sep 15;307(6):F718-26. doi: 10.1152/ajprenal.00372.2013. Epub 2014 Jul 23. Am J Physiol Renal Physiol. 2014. PMID: 25056349
-
The effects of glomerular and tubular renal progenitors and derived extracellular vesicles on recovery from acute kidney injury.Stem Cell Res Ther. 2017 Feb 7;8(1):24. doi: 10.1186/s13287-017-0478-5. Stem Cell Res Ther. 2017. PMID: 28173878 Free PMC article.
-
Protective effects of pioglitazone on renal ischemia-reperfusion injury in mice.J Surg Res. 2012 Nov;178(1):460-5. doi: 10.1016/j.jss.2012.01.012. Epub 2012 Apr 4. J Surg Res. 2012. PMID: 22507688
-
Ischemic acute kidney injury and klotho in renal transplantation.Clin Biochem. 2018 May;55:3-8. doi: 10.1016/j.clinbiochem.2018.03.022. Epub 2018 Mar 31. Clin Biochem. 2018. PMID: 29608890 Review.
-
Emerging therapeutic strategies for transplantation-induced acute kidney injury: protecting the organelles and the vascular bed.Expert Opin Ther Targets. 2019 Jun;23(6):495-509. doi: 10.1080/14728222.2019.1609451. Epub 2019 May 3. Expert Opin Ther Targets. 2019. PMID: 31022355 Review.
Cited by
-
Urinary NGAL Outperforms 99mTc-MAG3 Renography in Predicting DCD Kidney Graft Function.Transpl Int. 2025 May 12;38:13818. doi: 10.3389/ti.2025.13818. eCollection 2025. Transpl Int. 2025. PMID: 40421388 Free PMC article.
-
Molecular Mechanisms and Potential Therapeutic Targets of Ischemia-Reperfusion Injury in Kidney Transplantation.Curr Issues Mol Biol. 2025 Apr 17;47(4):282. doi: 10.3390/cimb47040282. Curr Issues Mol Biol. 2025. PMID: 40699682 Free PMC article. Review.
-
Ischemia Reperfusion Injury Triggers CXCL13 Release and B-Cell Recruitment After Allogenic Kidney Transplantation.Front Immunol. 2020 Aug 6;11:1204. doi: 10.3389/fimmu.2020.01204. eCollection 2020. Front Immunol. 2020. PMID: 32849490 Free PMC article.
-
Ischemia-Reperfusion Injury Reduces Long Term Renal Graft Survival: Mechanism and Beyond.EBioMedicine. 2018 Feb;28:31-42. doi: 10.1016/j.ebiom.2018.01.025. Epub 2018 Feb 2. EBioMedicine. 2018. PMID: 29398595 Free PMC article. Review.
-
A randomized double-blind, placebo-controlled clinical phase IIa trial on safety, immunomodulatory effects and pharmacokinetics of EA-230 during experimental human endotoxaemia.Br J Clin Pharmacol. 2019 Jul;85(7):1559-1571. doi: 10.1111/bcp.13941. Epub 2019 May 23. Br J Clin Pharmacol. 2019. PMID: 30919998 Free PMC article. Clinical Trial.
References
-
- Snoeijs MG, van Bijnen A, Swennen E, Haenen GR, Roberts LJ 2nd, et al. (2011) Tubular epithelial injury and inflammation after ischemia and reperfusion in human kidney transplantation. Ann Surg 253: 598–604. - PubMed
-
- Cooper JE, Wiseman AC (2013) Acute kidney injury in kidney transplantation. Curr Opin Nephrol Hypertens 22: 698–703. - PubMed
-
- Perico N, Cattaneo D, Sayegh MH, Remuzzi G (2004) Delayed graft function in kidney transplantation. Lancet 364: 1814–1827. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
